Afr. J. Parasitol. Mycol. Entomol. , 3(2), 15; doi:10.35995/ajpme03020015
Review
Ten Years of Seasonal Malaria Chemoprevention in Senegal: Scale-Up Process, Coverage, Tolerability—Ten Years of SMC in Senegal
1
Department of Parasitology-Mycology/Faculty of Medicine, Pharmacy and Odontology, Cheikh Anta Diop University, Dakar 5005, Senegal; fassiatht@yahoo.fr (F.T.); bellezenab@gmail.com (S.D.); mhadji2011@hotmail.com (A.M.); bfaye67@yahoo.fr (B.F.)
2
Department of Parasitology-Mycology/Medical Biology, UFR des Sciences de la Santé/Iba Der Thiam University, Thiès A967, Senegal; fabi.sall@univ-thies.sn (F.B.S.); mariepierrediouf@outlook.fr (M.P.D.); seckos3 @hotmail.com (A.S.); jlndiaye@univ-thies.sn (J.L.N.)
3
National Malaria Control Programme of Senegal, Dakar 25270, Senegal; mnzop5@yahoo.fr (M.N.); badou_gueye@hotmail.com (A.B.G.); kalystandeurnabi@yahoo.fr (S.N.K.); haril76@yahoo.fr (I.D.); drdocsene@yahoo.fr (D.S.)
4
Department of Parasitology-Mycology/Medical Biology, UFR des Sciences de la Santé/Gaston Berger University, Saint-Louis 234, Senegal; doudsow@yahoo.fr
*
Corresponding author: akhenmanga@yahoo.fr or isaacakhenaton1.manga@ucad.edu.sn; Tel.: +221-775885087
How to Cite: Manga, I.A.; Sall, F.B.; Diouf, M.P.; Tairou, F.; Seck, A.; Diop, S.; Mhadji, A.; Ndiop, M.; Gueye, A.B.; Kaly, S.N.; et al. Ten Years of Seasonal Malaria Chemoprevention in Senegal: Scale-Up Process, Coverage, Tolerability—Ten Years of SMC in Senegal. Afr. J. Parasitol. Mycol. Entomol. 2026, 3(2): 15; doi:10.35995/ajpme03020015.
Received: 4 November 2025 / Accepted: 15 May 2026 / Published: 29 May 2026
Abstract
:Background: Since 2013, Senegal has implemented seasonal malaria chemoprevention (SMC) with sulfadoxine–pyrimethamine plus amodiaquine (SPAQ) to reduce malaria among children under ten years of age. Over the past decade, SMC has become a cornerstone of malaria prevention, contributing to notable reductions in malaria incidence and mortality. Methods: This retrospective descriptive analysis of routine program data summarizes ten years of implementation, scaling up and adverse event monitoring of SMC in Senegal. Data were drawn from annual epidemiological bulletins and feedback reports from the National Malaria Control Programme (NMCP) between 2013 and 2021. These documents were analyzed to describe key stages of adoption, geographical expansion, and coverage trends. Tolerability and safety were assessed using adverse event (AE) reports documented by the national poison control center, which evaluates causality for suspected SPAQ-related events. Findings: Between 2013 and 2017, only the first daily dose of SPAQ was administered under directly observed treatment (DOT) by community health workers, while parents administered the remaining doses. Since 2019, all three doses have been administered under DOT. Coverage generally met or exceeded the national 95% target, although a temporary disruption occurred during health worker strikes in 2018. AE incidence remained very low (<0.5%), with most events being mild and only 19 serious cases reported over the ten-year period. Conclusion: Senegal’s decade-long SMC program achieved broad geographic expansion, sustained high coverage, and excellent tolerability. These results underscore the effectiveness of community-based delivery and the importance of sustained political and logistical support to consolidate malaria control gains.
Keywords:
Seasonal Malaria Chemoprevention (SMC); Senegal; community health workers; Malaria control1. Introduction
Despite significant progress in malaria control in sub-Saharan Africa, the disease remains a major public health concern, particularly among children living in areas with highly seasonal transmission patterns. Seasonal malaria chemoprevention (SMC), utilizing the combination of sulfadoxine–pyrimethamine and amodiaquine, has emerged as an effective strategy for reducing malaria-related morbidity and mortality.
Since its endorsement by the World Health Organization in 2012, SMC has been widely implemented across West African countries, including Senegal, with substantial reductions in malaria incidence reported [1,2,3,4,5,6,7,8]. More recently, the expansion of SMC recommendations to include older children reflects evolving evidence regarding malaria risk across different age groups. Notably, studies conducted in Senegal and Mali indicate that children aged 5–10 years remain particularly vulnerable [2,9,10,11,12,13].
However, the long-term success of SMC programs is contingent not only on their efficacy but also on the quality of implementation, the coverage achieved, and the tolerability under real-world conditions. Evidence from clinical trials, while reassuring, does not always fully capture the operational challenges associated with large-scale program deployment.
In Senegal, although SMC has been implemented for over a decade, comprehensive data on the scale-up process, coverage levels, and long-term tolerability remain limited—especially in light of the expanded target populations. Furthermore, while the adverse events associated with SMC are generally mild and transient, they may impact community adherence and overall program performance.
Additionally, emerging observations suggest potential variations in the occurrence of adverse events based on individual characteristics, such as sex, raising important questions related to pharmacovigilance and equity in intervention outcomes.
In this context, there is a clear need for robust and integrated evidence to evaluate the multiple dimensions of SMC implementation. This study was thus initiated to meet this requirement. Its objective was to describe the different stages of the scaling-up process, to determine coverage rates and to assess tolerance during the first ten years of implementation in Senegal.
2. Methodology
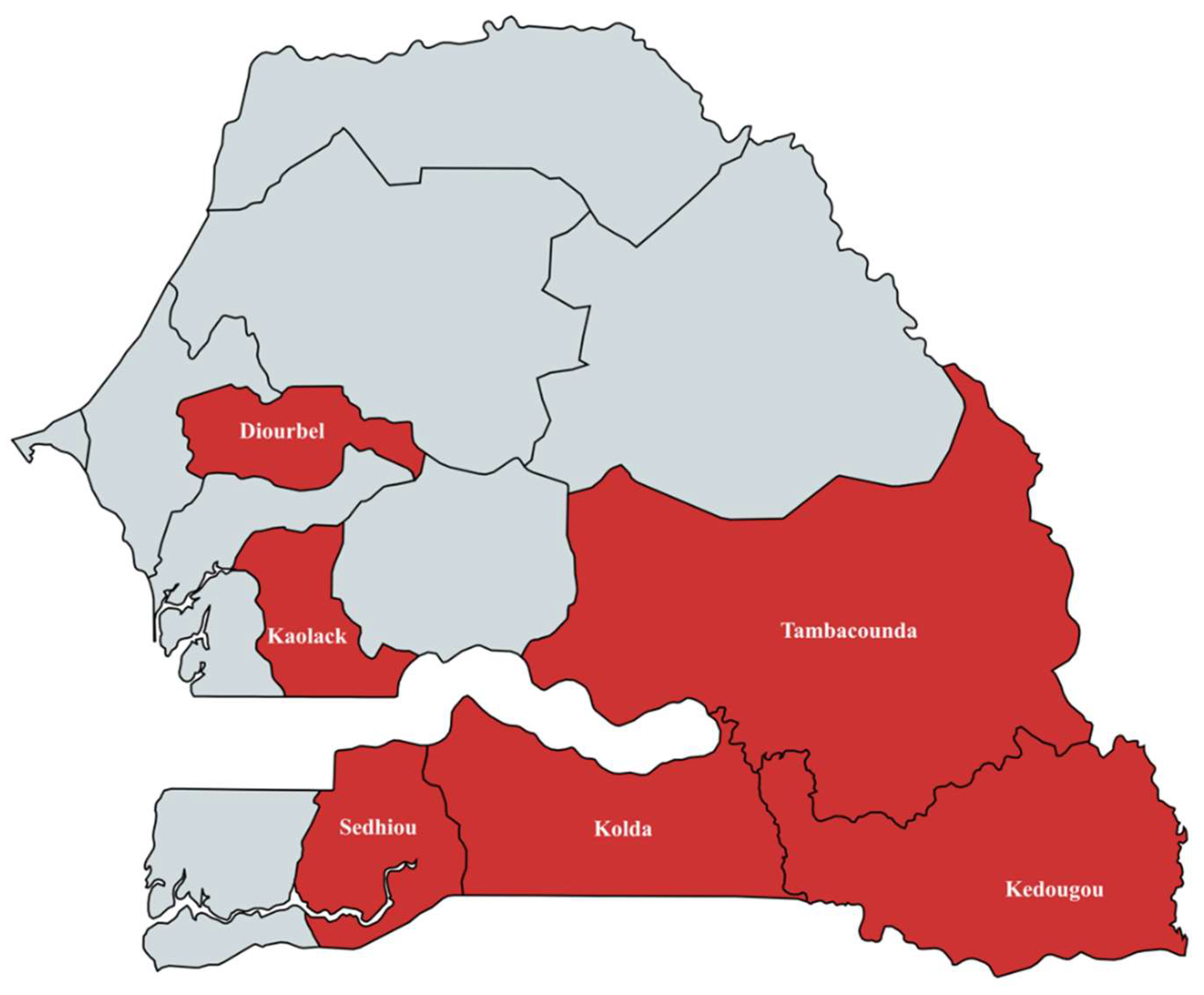
This study is a retrospective and secondary analysis of routine data from the National Malaria Control Programme (NMCP) in Senegal. It focused on information regarding SMC in Senegal from 2012 to 2021, covering the periods of its adoption, pilot implementation, and scaling up in parts of the country that meet the SMC eligibility criteria [1] (Figure 1).
To describe the key stages in the rollout of this malaria chemoprevention strategy in the country, reports from the various meetings that led to decisions on adoption, initial pilot-phase implementation and scaling up were analyzed. The data on SMC administration coverage analyzed in this study were drawn from all annual epidemiological bulletins [14,15,16,17,18,19,20,21] and official feedback reports for each SMC administration round under the NMCP covering the study period.
Only SMC coverage (proportion of children treated among all children recorded in the target population) data by administration round, reported in these bulletins, were extracted using Microsoft Excel (version 16.78.3) and subsequently analyzed using RStudio (version 2026.01.1+403).
SMC coverage rates were expressed as percentages and summarized by administration round and by implementation region across the study years. In addition, mean annual national coverage rates were compared using analysis of variance (ANOVA).
The study period was divided into two distinct phases. The first (2013–2017) corresponded to the period during which only the first dose of sulfadoxine–pyrimethamine plus amodiaquine (SPAQ) was administered under directly observed treatment (DOT) by community health workers, while the second and third doses were administered at home by caregivers on days 2 and 3. This phase also preceded the suspension of SMC implementation in 2018 due to nationwide health worker strikes. The second phase (2019–2021) corresponded to the resumption of SMC, during which all three doses were administered under directly observed treatment by community health workers. Mean coverage rates between these two periods were compared using Student’s t-test.
The level of statistical significance was set at p < 0.05 for both ANOVA and the t-test.
To assess the tolerability of SMC, adverse event reports submitted by regional medical authorities to the national poison control center responsible for causality assessment were reviewed. Data on adverse events were also extracted from annual epidemiological bulletins and post-campaign feedback reports for each administration round. All collected data were entered into Microsoft Excel (version 16.78.3). The number of reported adverse events (AEs) was extracted from these documents, and annual totals were calculated by summation. The annual AE incidence was then computed by dividing the total number of AEs by the total number of children treated during the corresponding year. Incidence rates were compared to the reference year 2013 (year of pilot phase) using the χ2 test with Yates’ continuity correction. Analyses were done using RStudio (version 2026.01.1+403).
Figure 1.
Regions where SMC was implemented in Senegal between 2013 and 2021.
3. Results
3.1. Development of SMC Scale-Up in Senegal
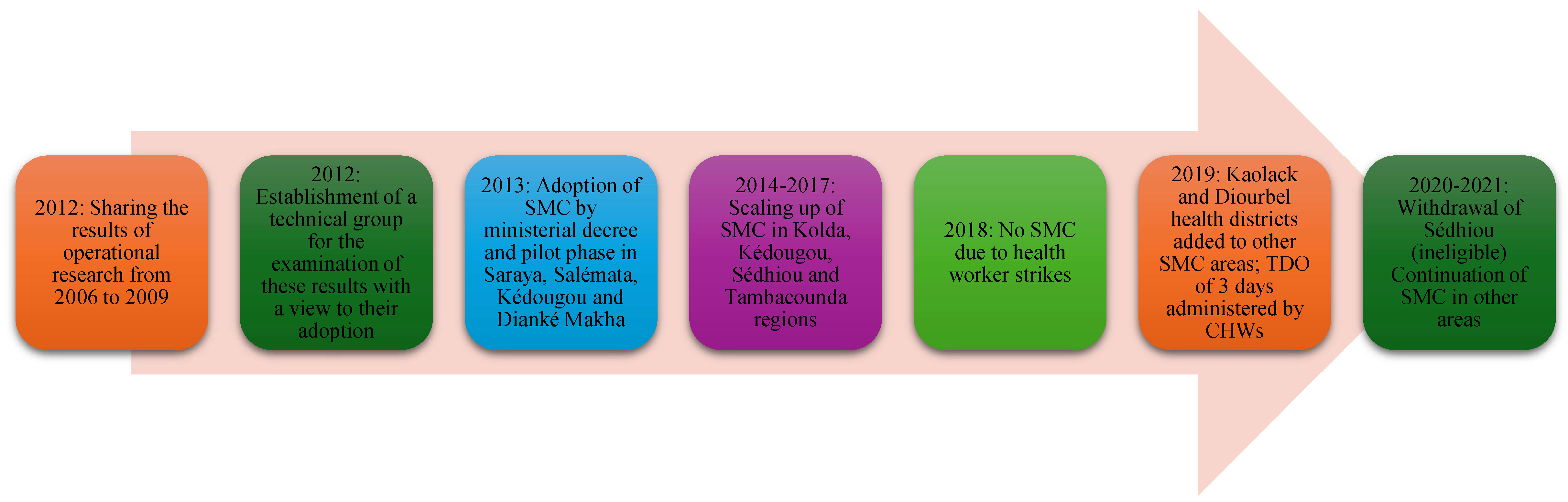
In 2012, after analyzing the malaria situation and disseminating the results of operational research on SMC conducted in the country [5,9,10,12,22], the Senegalese health authorities decided to adopt SMC as recommended by the WHO [2]. A ministerial note (003685/MSAS/DS/DLM/PNLP 11 May 2012, unpublished) was issued to establish a technical group to determine the target population, implementation zone and the most appropriate method of administering the SMC in Senegal.
This strategy was then piloted in November and December 2013 in three districts (Kédougou, Salémata and Saraya) of the Kédougou region and in the Dianké Makha district of Tambacounda. During this pilot phase, only two monthly rounds were administered.
In 2014, the regions of Kolda and Sédhiou and the six other districts of Tambacounda were added to the areas where SMC had been implemented the previous year. This year, the SMC campaign was carried out in three monthly rounds. From 2015 to 2017, for each annual campaign, there were four monthly rounds for the Kédougou region and three rounds for the others. In 2018, SMC was not conducted in the designated areas in Senegal due to health worker strikes that paralyzed the entire health system. In 2019, the districts of Diourbel and Kaolack were added to the country’s former SMC implementation zones. Finally, in 2020, the Sédhiou region was removed from eligible areas (Figure 2).
In Senegal, SMC is administered by community health workers (CHWs) using a door-to-door approach. Up to and including 2017, administration was carried out under directly observed treatment (DOT) by CHWs for the dose (SP+AQ) on day 1 (D1). Doses (AQ only) on days 2 and 3 (D3) were administered by parents/caregivers. To optimize coverage of the full course of treatment, the NMCP decided, after analyzing the data, that from 2019 onwards, all three doses of SMC would be administered under the DOT of the CHWs.
Figure 2.
Scaling up of SMC in Senegal between 2012 and 2021.
3.2. SMC Coverage Rates in Senegal Between 2013 and 2021
The coverage rates achieved varied by region, administration round and year. For example, in the Kédougou region, the national coverage target of 95% was not reached in the first rounds of 2013 (92.5%), 2014 (91%), 2017 (90%) and 2019 (93.9%). In the same region, for the second rounds, this target was only met or exceeded in 2013 and 2014, with coverage rates of 95.4% and 101% respectively. For the third rounds, coverage rates of 95% or higher were only achieved in 2014 (101%) and 2021 (95.4%). The fourth rounds in Kédougou with a coverage rate above the national target were in 2019 and 2021. Similar variations in SMC coverage rates between rounds and years were also observed in the other regions where the strategy was administrated. In the new regions of Kaolack and Diourbel, which have been included since 2019, the target was only reached in the third round of 2020 in Kaolack (95.2%) and in the second and third rounds of 2021 in Diourbel, where coverage was 95.2% and 95.3% respectively (Table 1).

Table 1.
SMC coverage in Senegal by round and region of implementation between 2013 and 2021.
| Year | KEDOUGOU | TAMBACOUNDA | KOLDA | SEDHIOU | DIOURBEL | KAOLACK | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1st rd | 2nd rd | 3rd rd | 4th rd | 1st rd | 2nd rd | 3rd rd | 1st rd | 2nd rd | 3rd rd | 1st rd | 2nd rd | 3rd rd | 1st rd | 2nd rd | 3rd rd | 1st rd | 2nd rd | 3rd rd | |
| 2013 | 92.5 | 95.4 | NA | NA | 93 | 97 | NA | NA | NA | NA | NA | NA | NA | Not yet included in SMC implementation area | |||||
| 2014 | 91 | 101 | 101 | NA | 96 | 97 | 99 | 97.3 | 99.9 | 98.1 | 95 | 98 | 99 | ||||||
| 2015 | 96 | 93 | 92 | 94 | 97 | 96 | 95 | 99 | 98 | 97 | 97 | 94 | 99 | ||||||
| 2016 | 97 | 95 | 94.4 | 95 | 96 | 96.7 | 97 | 98 | 98.1 | 98 | 98 | 97.7 | 99 | ||||||
| 2017 | 90 | 93 | 90 | 90.8 | 95 | 95 | 92.5 | 98 | 96 | 93 | 98 | 95 | 95.1 | ||||||
| 2018 | Staff strikes → No SMC campaign | ||||||||||||||||||
| 2019 | 93.9 | 94.6 | 94.1 | 95.3 | 97 | 97 | 91 | 89.6 | 86.9 | 89.2 | 96.9 | 96.3 | 86 | 87.2 | 90.3 | 88 | 72.6 | 95 | |
| 2020 | 96.4 | 94.9 | 93.9 | 94.9 | 96.4 | 97 | 97.4 | 97.3 | 97.5 | 97.8 | Exit from SMC zone because region no longer eligible | 89.1 | 94.7 | 100 | 88.5 | 93.5 | 95.2 | ||
| 2021 | 95.8 | 94.3 | 95.4 | 95.4 | 97.7 | 98.2 | 97.2 | 98 | 98.3 | 98.3 | 94.9 | 95.2 | 95.3 | 94.1 | 94.7 | 93.2 | |||
rd: Round; NA: Not Applicable. SMC was only administered in two rounds in 2013 in Kedougou and Tambacounda.
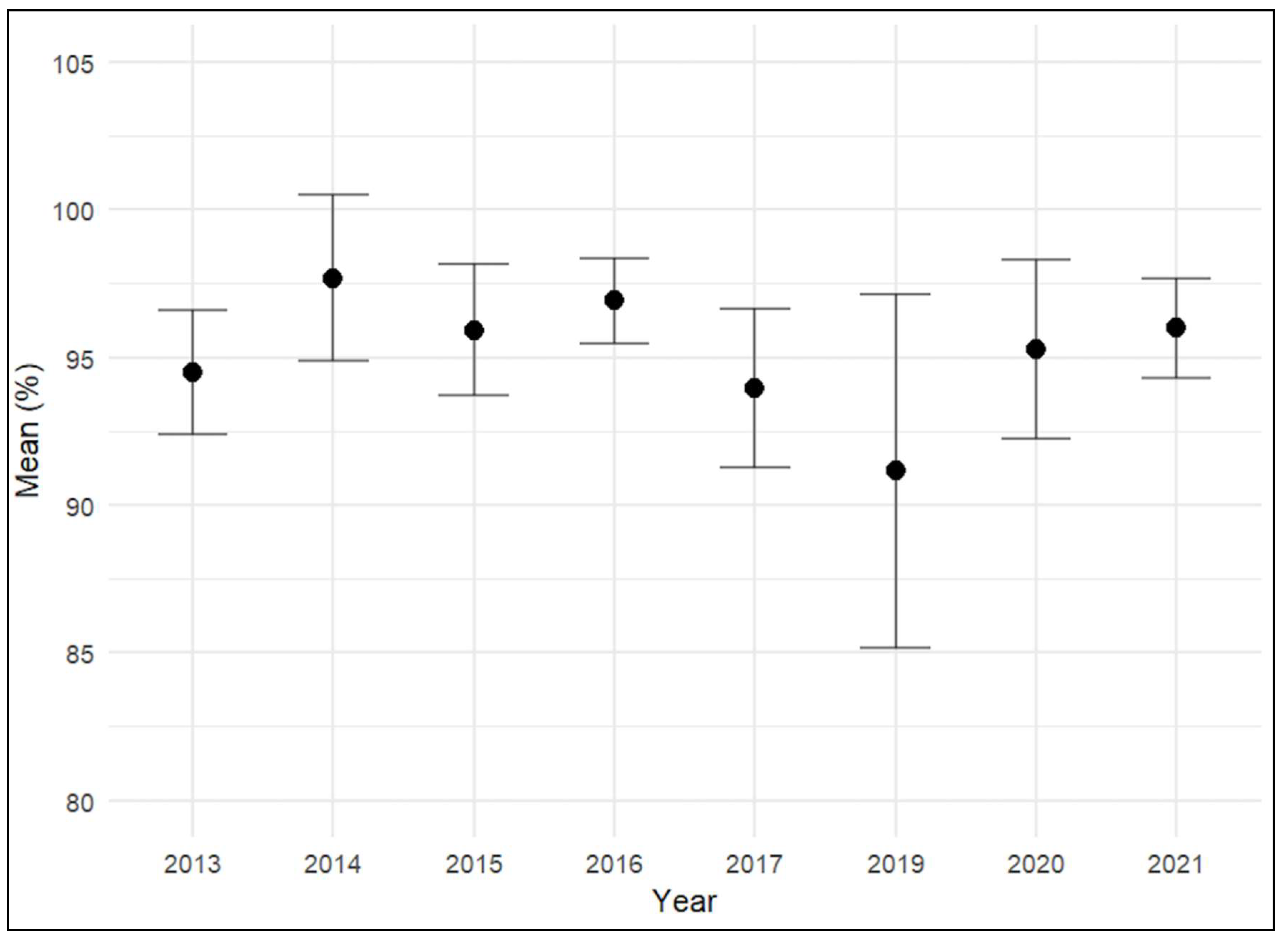
The analysis of the annual trend in the mean coverage of SMC revealed variations in coverage levels over the study period. Annual mean coverage ranged overall from approximately 91% to 98%, with relatively high levels observed between 2013 and 2016, peaking around 2014. A decline was observed in 2017, followed by a more pronounced decrease in 2019, which recorded the lowest mean coverage. Subsequently, a gradual increase was noted in 2020 and 2021.
Statistical analysis using ANOVA showed a highly significant overall difference in mean coverage across the years (p < 0.001) (Figure 3).
Pairwise comparisons of mean seasonal malaria chemoprevention (SMC) coverage across different years revealed that most differences were not statistically significant after adjusting for multiple comparisons. However, a significant decrease in coverage was noted in 2019 compared to previous years, particularly when contrasted with 2014 (−6.53; 95% CI: −10.35 to −2.72; p < 0.001), 2015 (−4.76; 95% CI: −8.49 to −1.04; p = 0.003), and 2016 (−5.75; 95% CI: −9.48 to −2.03; p < 0.001). In contrast, a significant increase in coverage was observed in the years following 2019, with higher values recorded in 2020 (difference: 4.12; 95% CI: 0.60 to 7.64; p = 0.010) and 2021 (difference: 4.84; 95% CI: 1.32 to 8.36; p = 0.001) compared to 2019. No statistically significant differences were found in most other year-to-year comparisons (Appendix A).
Figure 3.
Trend in mean annual coverage between 2013 and 2021.
- -
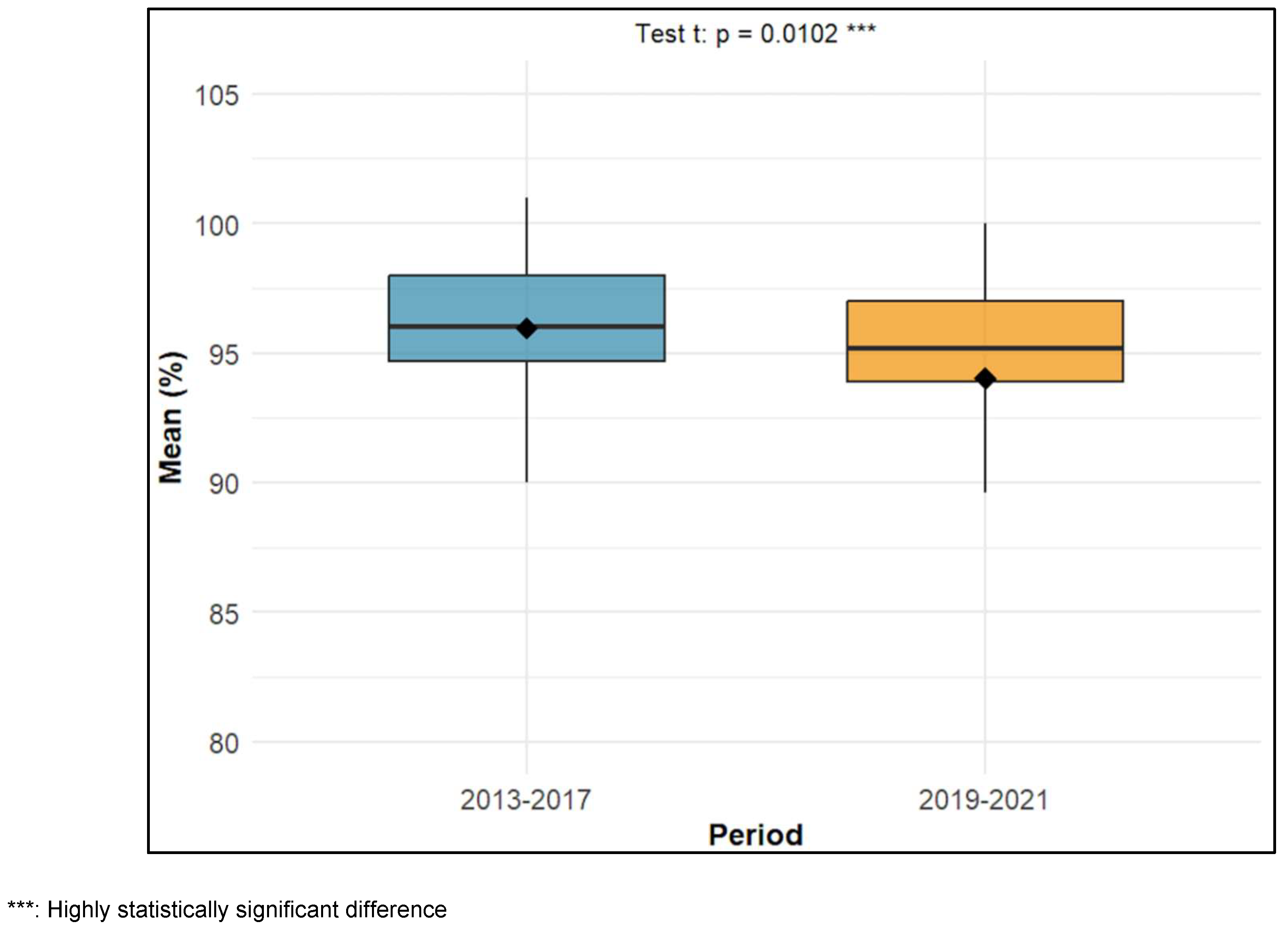
- Comparison of the mean coverage of SMC between 2013 and 2017 (DOT on day 1 only) and 2019 and 2021 (DOT over three days)
The mean coverage of seasonal malaria chemoprevention (SMC) was 95.8% (±1.58) during the 2013–2017 period. For the 2019–2021 period, the mean coverage was 94.1% (±2.6). Comparison of the means showed a statistically significant difference between the two periods (t-test → p = 0.0102) (Figure 4).
Figure 4.
Comparison of mean between 2013 and 2017 DOT only day 1) and 2019 and 2021 (DOT over 3 days).
Figure 4.
Comparison of mean between 2013 and 2017 DOT only day 1) and 2019 and 2021 (DOT over 3 days).
3.3. Adverse Events Reported
Between 2013 and 2021, a total of 5797 adverse events (AEs) were reported for 4,740,701 children treated, corresponding to an overall incidence rate of 0.12%. The annual incidence rate varied considerably over the period, ranging from 0.01% in 2017 to 0.33% in 2015. The year 2015 recorded the highest number of AEs (n = 2039) as well as the highest incidence rate (0.33%). After a decline in 2016 (0.05%) and 2017 (0.01%), incidence rates increased to 0.17% in 2019 and 0.18% in 2020, before decreasing to 0.07% in 2021. A significant increase in the incidence rate was observed in 2015 (0.328%, p < 0.0001), 2019 (0.167%, p = 0.017), and 2020 (0.175%, p = 0.010) compared to 2013. In contrast, the incidence rates in 2014 (0.054%, p = 0.076), 2016 (0.051%, p = 0.262), 2017 (0.012%, p = 0.338), and 2021 (0.071%, p = 0.092) were not significantly different from that of 2013 (Table 2).
Table 2.
Incidence of adverse events reported during SMC campaigns between 2013 and 2021 in Senegal.
Table 2.
Incidence of adverse events reported during SMC campaigns between 2013 and 2021 in Senegal.
| Year | Number of AEs Reported | Number of Children Treated | Incidence Rate | χ2 (Yates) | p-Value |
|---|---|---|---|---|---|
| 2013 | 13 | 59,480 | 0.02% | - | - |
| 2014 | 335 | 614,785 | 0.05% | 3.14 | 0.07 |
| 2015 | 2039 | 620,877 | 0.33% | 19.85 | <0.0001 |
| 2016 | 318 | 624,802 | 0.05% | 1.26 | 0.26 |
| 2017 | 78 | 627,729 | 0.01% | 0.92 | 0.33 |
| 2018 | NA | NA | NA | NA | NA |
| 2019 | 1348 | 808,211 | 0.17% | 5.67 | 0.01 |
| 2020 | 1149 | 655,792 | 0.18% | 6.69 | 0.01 |
| 2021 | 517 | 729,025 | 0.07% | 2.84 | 0.09 |
| Total | 5797 | 4,740,701 | 0.12% | - | - |
NA: Not applicable because there was no SMC in 2018.
The vast majority of AEs were of minor severity (n = 5778), with only 19 major AEs, occurring predominantly in 2021 (n = 11). The distribution by sex was balanced, with 3013 AEs reported in boys and 2679 in girls. Similarly, the distribution by age group showed 2,956 AEs in children aged ≤5 years and 2835 in those aged >5 years. Substantial geographic variation was observed, with the highest number of AEs reported in Kaolack (n = 1814), Sédhiou (n = 1456), and Kolda (n = 1149), while fewer AEs were reported in Diourbel (n = 240), Kédougou (n = 480), and Tambacounda (n = 658). The marked increase in the number of AEs in 2015 (n = 2039) and again in 2019 (n = 1348) and 2020 (n = 1149) may reflect intensified surveillance, program expansion, or increased exposure during these periods (Table 3).
Table 3.
Distribution of AEs by severity, sex, age group and region, by year.
| 2013 (N = 13) | 2014 (N = 335) | 2015 (N = 2039) | 2016 (N = 318) | 2017 (N = 78) | 2019 (N = 1348) | 2020 (N = 1149) | 2021 (N = 517) | Overall (N = 5797) | |
|---|---|---|---|---|---|---|---|---|---|
| Severity of AEs | |||||||||
| - Minor | 13 | 333 | 2039 | 318 | 77 | 1343 | 1149 | 506 | 5778 |
| - Major | 0 | 2 | 0 | 0 | 1 | 5 | 0 | 11 | 19 |
| Sex * | |||||||||
| - Boys | 7 | 194 | 1027 | 186 | 42 | 705 | 598 | 254 | 3013 |
| - Girls | 6 | 127 | 1011 | 130 | 36 | 610 | 513 | 246 | 2679 |
| Age group * | |||||||||
| - ≤5 years | 8 | 102 | 1229 | 140 | 38 | 634 | 541 | 264 | 2956 |
| - >5 years | 5 | 233 | 810 | 178 | 40 | 708 | 608 | 253 | 2835 |
| Region | |||||||||
| - Kédougou | 13 | 139 | 39 | 46 | 0 | 71 | 120 | 52 | 480 |
| - Tambacounda | 0 | 143 | 36 | 10 | 63 | 125 | 233 | 48 | 658 |
| - Sédhiou | 0 | 1 | 1174 | 194 | 0 | 87 | - | - | 1456 |
| - Kolda | 0 | 52 | 790 | 68 | 15 | 83 | 93 | 48 | 1149 |
| - Diourbel | - | - | - | - | - | 39 | 36 | 165 | 240 |
| - Kaolack | - | - | - | - | - | 943 | 667 | 204 | 1814 |
* A total of 105 missing data points on sex and 6 missing data points on age; (-) indicates years during which the region was not yet included or excluded (Sédhiou).
4. Discussion
This study provides a comprehensive analysis of the first ten years of seasonal malaria chemoprevention (SMC) implementation in Senegal. It documents the scale-up process, coverage achievements, and tolerability profile. Several limitations should be acknowledged: reliance on routine programmatic data subject to reporting issues, absence of 2018 data, potential overestimation of coverage due to denominator inaccuracies, and lack of clinical outcome data.
The findings of this study demonstrate that SMC has been successfully scaled from an initial pilot in two districts in 2013 to nationwide coverage in eligible regions, with sustained high coverage rates and a very low overall incidence of adverse events. These results reinforce the feasibility and effectiveness of community-based SMC delivery within a routine health system context [2,4].
- Scale-up process and implementation milestones
The rollout of seasonal malaria chemoprevention (SMC) in Senegal over time followed the World Health Organization (WHO) recommendations for implementing this strategy [1,2]. Indeed, after a pilot phase with two administration cycles in 2013 in the three health districts of the Kédougou region and in Dianké Makha (Tambacounda), the intervention was progressively expanded to other eligible areas, with the number of cycles adapted to the local context. The continuous evaluation of this strategy also led to the removal of the Sédhiou region in 2020 from SMC-eligible areas, as it no longer met the eligibility criteria.
The non-administration of seasonal malaria chemoprevention (SMC) in 2018 due to a health worker strike highlights the fragility of our health system. The absence of alternative mechanisms in such situations threatens all the efforts made to sustain the gains achieved by the country, particularly in malaria control. This observation is especially relevant given the growing emphasis on health system resilience [3,13]. Moreover, this study demonstrates, through the coverage rates achieved after this interruption, the capacity of the Senegalese health system to recover and rebound [4].
The transition from DOT of only the first dose to three-day DOT represents a major programmatic shift and further reflects the continuous evaluation of SMC and the commitment to ensuring that children receive the full course of treatment. This change may also explain the increase in adverse event (AE) reporting following the introduction of three-day DOT, as closer supervision by community health workers likely improved the detection and reporting of AEs [11,12].
- Coverage achievements and challenges
CPS coverage rates in Senegal during the study period varied over time and across regions, but consistently hovered around the 95% target, as shown by the national annual averages, which ranged from 91.7% to 97.5%. The achievement of these coverage levels could be explained by community engagement, door-to-door delivery, strong political commitment, and thorough training of CHWs [8,14,15,16]. Although coverage levels were generally high, they varied across years and regions, with both declines and increases observed. The declines could be explained by the implementation of the full three-day directly observed treatment (DOT), suggesting a trade-off between treatment completion and coverage efficiency [17]. They may also be attributed to the expansion of the program to new regions with limited experience in implementation, as well as the lingering effects of the 2018 health worker strikes. Coverage rates exceeding 100% suggest potential inaccuracies in target population estimates, a common phenomenon in administrative coverage data [18].
Senegal’s coverage rates (91.7–97.5%) compare favorably with those of other West African countries. Niger achieved 85.7% in 2016 [6], the ACCESS SMC project reported average monthly coverage of 76.4% in 2015 and 74.8% in 2016 across seven countries [23], and Mali achieved 77% average first-dose coverage [24]. The door-to-door delivery approach in Senegal likely explains these higher rates [14,25].
- Tolerability and adverse event profile
The overall AE incidence in this study was very low and the majority were minor with only 19 major AEs reported over ten years, all of which resolved after hospital care. These findings are consistent with previous studies in Senegal, which reported AE incidences of 0.1–0.2% and very few serious events [14,19]. Annual AE incidence ranged from 0.01% to 0.33%. The peak observed in 2015 coincides with program expansion, while the increases in 2019 and 2020 align with the transition to three-day DOT.
Comparable findings have been reported in other countries. In Niger, no serious AEs were reported in 2016 [6], and in Mali, 131 AEs were reported in 104 children between 2015 and 2016, with the majority being mild [20,21].
The geographic distribution showed higher AE numbers in Kaolack, Sédhiou, and Kolda, likely reflecting the larger number of children treated. However, the complete absence of reported AEs in certain regions despite high coverage suggests underreporting, highlighting the need for strengthened pharmacovigilance [22]. The balanced distribution by sex and age group supports the expanded target population to include children up to 10 years of age [2].
5. Conclusions
The implementation of SMC in Senegal has been dynamic. It began with a pilot phase before being scaled up in four regions in the south-east of the country. Over the decade, new areas have been added to the SMC program while one area that no longer met WHO eligibility criteria has been phased out. Community involvement, along with a door-to-door strategy, has led to high coverage rates for this well-tolerated strategy in Senegal.
Author Contributions
Study design: I.A.M. and J.L.N. Data collection and analysis: I.A.M., J.L.N., A.S., F.T., A.M., F.B.S., M.P.D. and S.D. Writing of the first draft of the manuscript: I.A.M., S.D., F.B.S., F.T., M.P.D. and A.S. Support and correction of the article: M.N., A.B.G., S.N.K., I.D., D.S. (Doudou Sow), J.L.N., B.F. and A.M. Supervision: D.S. (Doudou Sow), D.S. (Doudou Sène), B.F. and J.L.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
This article is dedicated to the late Professor Jean Louis Abdourahim NDIAYE, whose pioneering contributions were instrumental in shaping the World Health Organization’s recommendation of seasonal malaria chemoprevention (SMC). In Senegal, he played a pivotal role in the monitoring and evaluation of this strategy. The present work reflects part of the outcomes of his extensive research on SMC in Senegal and aims to support the continued integration of this intervention within the country’s malaria control efforts.
Acknowledgments
The authors would like to thank the following people and organizations: The Ministry of Health and Public Hygiene, the malaria control program, the populations of the regions where SMC is implemented, community actors and health personnel responsible for administering SMC, and the staff of the Parasitology-Mycology laboratories at the universities of Dakar, Thiès and Saint Louis.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Appendix A
Table A1.
Comparison of national overall coverage by year.
| Comparison | Coverage Difference | 95% CI | Adjusted p-Value |
|---|---|---|---|
| 2014 vs. 2013 | 3.22 | [−2.69; 9.13] | 0.696 |
| 2015 vs. 2013 | 1.45 | [−4.41; 7.30] | 0.994 |
| 2016 vs. 2013 | 2.44 | [−3.41; 8.29] | 0.900 |
| 2017 vs. 2013 | −0.52 | [−6.37; 5.33] | 0.999 |
| 2019 vs. 2013 | −3.31 | [−8.97; 2.34] | 0.612 |
| 2020 vs. 2013 | 0.81 | [−4.92; 6.53] | 0.999 |
| 2021 vs. 2013 | 1.53 | [−4.20; 7.25] | 0.991 |
| 2015 vs. 2014 | −1.77 | [−5.87; 2.33] | 0.882 |
| 2016 vs. 2014 | −0.78 | [−4.87; 3.32] | 0.999 |
| 2017 vs. 2014 | −3.74 | [−7.84; 0.36] | 0.101 |
| 2019 vs. 2014 | −6.53 | [−10.35; −2.72] | <0.001 |
| 2020 vs. 2014 | −2.41 | [−6.32; 1.50] | 0.547 |
| 2021 vs. 2014 | −1.69 | [−5.60; 2.22] | 0.881 |
| 2016 vs. 2015 | 0.99 | [−3.02; 5.01] | 0.994 |
| 2017 vs. 2015 | −1.97 | [−5.98; 2.05] | 0.795 |
| 2019 vs. 2015 | −4.76 | [−8.49; −1.04] | 0.003 |
| 2020 vs. 2015 | −0.64 | [−4.46; 3.18] | 0.999 |
| 2021 vs. 2015 | 0.08 | [−3.75; 3.90] | 1.000 |
| 2017 vs. 2016 | −2.96 | [−6.98; 1.05] | 0.313 |
| 2019 vs. 2016 | −5.75 | [−9.48; −2.03] | <0.001 |
| 2020 vs. 2016 | −1.63 | [−5.46; 2.19] | 0.887 |
| 2021 vs. 2016 | −0.92 | [−4.74; 2.91] | 0.995 |
| 2019 vs. 2017 | −2.79 | [−6.52; 0.93] | 0.293 |
| 2020 vs. 2017 | 1.33 | [−2.50; 5.15] | 0.960 |
| 2021 vs. 2017 | 2.05 | [−1.78; 5.87] | 0.714 |
| 2020 vs. 2019 | 4.12 | [0.60; 7.64] | 0.010 |
| 2021 vs. 2019 | 4.84 | [1.32; 8.36] | 0.001 |
| 2021 vs. 2020 | 0.72 | [−2.90; 4.34] | 0.999 |
References
- Organisation Mondiale de la Santé. Chimioprévention du Paludisme Saisonnier par Administration de Sulfadoxine-Pyriméthamine et D’amodiaquine aux Enfants: Guide de Terrain. Juillet 2013. Available online: https://iris.who.int/bitstream/handle/10665/85727/9789242504736_fre.pdf?sequence=1 (accessed on 17 April 2024).
- Organisation Mondiale de la Santé. Chimioprévention du Paludisme Saisonnier par Administration de Sulfadoxine-Pyriméthamine et D’amodiaquine aux Enfants: Guide de Terrain. Deuxième Edition. 26 Mai 2023|Manuel. Available online: https://www.who.int/fr/publications-detail/9789240073692 (accessed on 17 April 2024).
- Cairns, M.; Ceesay, S.J.; Sagara, I.; Zongo, I.; Kessely, H.; Gamougam, K.; Diallo, A.; Ogboi, J.S.; Moroso, D.; Van Hulle, S.; et al. Effectiveness of seasonal malaria chemoprevention (SMC) treatments when SMC is implemented at scale: Case–control studies in 5 countries. PLoS Med. 2021, 18, e1003727. [Google Scholar] [CrossRef] [PubMed]
- ACCESS-SMC Partnership. Effectiveness of seasonal malaria chemoprevention at scale in west and central Africa: An observational study. Lancet 2020, 396, 1829–1840, PMCID:PMC7718580. [Google Scholar] [CrossRef] [PubMed]
- Cissé, B.; Sokhna, C.; Boulanger, D.; Milet, J.; Bâ, E.H.; Richardson, K.; Hallett, R.; Sutherland, C.; Simondon, K.; Simondon, F.; et al. Seasonal intermittent preventive treatment with artesunate and sulfadoxine-pyrimethamine for prevention of malaria in Senegalese children: A randomised, placebo-controlled, double-blind trial. Lancet 2006, 367, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Manga, I.A.; Tairou, F.; Seck, A.; Kouevidjin, E.; Sylla, K.; Sow, D.; Gueye, A.B.; Ba, M.; Ndiaye, M.; Tine, R.C.; et al. Effectiveness of seasonal malaria chemoprevention administered in a mass campaign in the Kedougou region of Senegal in 2016: A case-control study. Wellcome Open Res. 2023, 7, 216. [Google Scholar] [CrossRef] [PubMed]
- Dicko, A.; Diallo, A.I.; Tembine, I.; Dicko, Y.; Dara, N.; Sidibe, Y.; Santara, G.; Diawara, H.; Conaré, T.; Djimde, A.; et al. Intermittent Preventive Treatment of Malaria Provides Substantial Protection against Malaria in Children Already Protected by an Insecticide-Treated Bednet in Mali: A Randomised, Double-Blind, Placebo-Controlled Trial. PLoS Med. 2011, 8, e1000407. [Google Scholar] [CrossRef] [PubMed]
- Konaté, D.; Diawara, S.I.; Touré, M.; Diakité, S.A.; Guindo, A.; Traoré, K.; Diarra, A.; Keita, B.; Thiam, S.; Keita, M.; et al. Effect of routine seasonal malaria chemoprevention on malaria trends in children under 5 years in Dangassa, Mali. Malar. J. 2020, 19, 137. [Google Scholar] [CrossRef] [PubMed]
- Ndiaye, Y.; Ndiaye, J.L.; Cisse, B.; Blanas, D.; Bassene, J.; Manga, I.A.; Ndiath, M.; Faye, S.L.; Bocoum, M.; Ndiaye, M.; et al. Community case management in malaria: Review and perspectives after four years of operational experience in Saraya district, south-east Senegal. Malar. J. 2013, 12, 240. [Google Scholar] [CrossRef] [PubMed]
- Tine, R.C.; Ndour, C.T.; Faye, B.; Cairns, M.; Sylla, K.; Ndiaye, M.; Ndiaye, J.L.; Sow, D.; Cisse, B.; Magnussen, P.; et al. Feasibility, safety and effectiveness of combining home based malaria management and seasonal malaria chemoprevention in children less than 10 years in Senegal: A cluster-randomised trial. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Cissé, B.; Ba, E.H.; Sokhna, C.; NDiaye, J.L.; Gomis, J.F.; Dial, Y.; Pitt, C.; NDiaye, M.; Cairns, M.; Faye, E.; et al. Effectiveness of Seasonal Malaria Chemoprevention in Children under Ten Years of Age in Senegal: A Stepped-Wedge Cluster-Randomised Trial. PLoS Med. 2016, 13, e1002175. [Google Scholar] [CrossRef] [PubMed]
- Bâ, E.H.; Pitt, C.; Dial, Y.; Faye, S.L.; Cairns, M.; Faye, E.; Ndiaye, M.; Gomis, J.F.; Faye, B.; Ndiaye, J.L.; et al. Implementation, coverage and equity of large-scale door-to-door delivery of Seasonal Malaria Chemoprevention (SMC) to children under 10 in Senegal. Sci. Rep. 2018, 8, 5489. [Google Scholar] [CrossRef] [PubMed]
- Diawara, S.I.; Konaté, D.; Kayentao, K.; Mihigo, J.; Shaffer, J.G.; Sangare, M.; Ndabamenye, P.; Swedberg, E.; Garg, L.W.; Gamache, N.; et al. Effect of seasonal malaria chemoprevention in children between 5 and 9 years old in Kita and Bafoulabe districts, Mali. Parasite Epidemiol. Control 2022, 18, e00258. [Google Scholar] [CrossRef] [PubMed]
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2014 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/BULLETIN-EPIDEMIOLOGIQUE-ANNUEL-2014-DU-PALUDISME-AU-SENEGAL-vf.pdf (accessed on 17 April 2024).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2015 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-ANNUEL-2015-du-Paludisme-au-SENEGAL-vf.pdf (accessed on 17 April 2024).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2016 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-Annuel-2016-du-Paludisme-au-Senegal-VF.pdf (accessed on 23 April 2024).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2017 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-ANNUEL-2017-du-Paludisme-au-SENEGAL-VFINALE.pdf (accessed on 16 April 2024).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2018 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-ANNUEL-2018-du-Paludisme-au-SENEGAL-vfe.pdf (accessed on 17 April 2024).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2019 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-ANNUEL-2019-du-Paludisme-au-SENEGAL-VFinale.pdf (accessed on 20 December 2021).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2020 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-ANNUEL-2020-du-Paludisme-au-SENEGAL-VFinale.pdf (accessed on 19 April 2024).
- Programme National de Lutte Contre le Paludisme. Bulletin Epidémiologique Annuel 2021 du Paludisme au Sénégal. Available online: https://pnlp.sn/wp-content/uploads/2020/11/Bulletin-Epidemiologique-ANNUEL-2021-du-Paludisme-au-SENEGAL-VFinale.pdf (accessed on 19 April 2024).
- NDiaye, J.L.; Cissé, B.; Ba, E.H.; Gomis, J.F.; Ndour, C.T.; Molez, J.F.; Fall, F.B.; Sokhna, C.; Faye, B.; Kouevijdin, E.; et al. Safety of Seasonal Malaria Chemoprevention (SMC) with Sulfadoxine-Pyrimethamine plus Amodiaquine when Delivered to Children under 10 Years of Age by District Health Services in Senegal: Results from a Stepped-Wedge Cluster Randomized Trial. PLoS ONE 2016, 11, e0162563. [Google Scholar]
- Manga, I.A. Impacts de la Mise à L’échelle de la Chimioprévention du Paludisme Saisonnier Administrée en Campagne de Masse Chez Les Enfants de Moins de 10 ans au sud du Sénégal. D’exercice de Médecine Thèse. Université Cheikh Anta Diop, Dakar, Senegal, 2016. Available online: http://bibnum.ucad.sn/viewer.php?c=thm&d=thm%5f2016%5f0444 (accessed on 6 August 2024).
- Ndiaye, J.L.A.; Ndiaye, Y.; Ba, M.S.; Faye, B.; Ndiaye, M.; Seck, A.; Tine, R.; Thior, P.M.; Atwal, S.; Beshir, K.; et al. Seasonal malaria chemoprevention combined with community case management of malaria in children under 10 years of age, over 5 months, in south-east Senegal: A cluster-randomised trial. PLoS Med. 2019, 16, e1002762. [Google Scholar] [CrossRef] [PubMed]
- Sesay, S.; Milligan, P.; Touray, E.; Sowe, M.; Webb, E.L.; Greenwood, B.M.; Bojang, K.A. A trial of intermittent preventive treatment and home-based management of malaria in a rural area of The Gambia. Malar. J. 2011, 10, 2. [Google Scholar] [CrossRef] [PubMed]
© 2026 Copyright by Authors. Licensed as an open access article using a CC BY 4.0 license.