Afr. J. Parasitol. Mycol. Entomol. , 4(1), 1; doi:10.35995/ajpme04010001
Article
Assessment of the Therapeutic Effectiveness of the Combination of Oral Ivermectin and Azithromycin in the Treatment of Head Lice Infestations in Rural Areas of Senegal
Georges Diatta 1 ,
Dame Ndiaye 1,
Nafissatou Diagne 1,
Broaly Richmond Tra Bi 1,
Oleg Mediannikov 2,3,
Alissa Hammoud 2,3,
El Hadji Ba 1,
Aldiouma Diallo 1,
Hubert Bassene 1,
Muriel Vray 4,
Sébastien Cortaredona 3,5,
Philippe Parola 3,5,
Didier Raoult 3
and
Cheikh Sokhna 1,3,5,*
,
Dame Ndiaye 1,
Nafissatou Diagne 1,
Broaly Richmond Tra Bi 1,
Oleg Mediannikov 2,3,
Alissa Hammoud 2,3,
El Hadji Ba 1,
Aldiouma Diallo 1,
Hubert Bassene 1,
Muriel Vray 4,
Sébastien Cortaredona 3,5,
Philippe Parola 3,5,
Didier Raoult 3
and
Cheikh Sokhna 1,3,5,*
,
Dame Ndiaye 1,
Nafissatou Diagne 1,
Broaly Richmond Tra Bi 1,
Oleg Mediannikov 2,3,
Alissa Hammoud 2,3,
El Hadji Ba 1,
Aldiouma Diallo 1,
Hubert Bassene 1,
Muriel Vray 4,
Sébastien Cortaredona 3,5,
Philippe Parola 3,5,
Didier Raoult 3
and
Cheikh Sokhna 1,3,5,*
1
Maladies Infectieuses Négligées Émergentes au Sud (MINES), Campus International Institut de Recherche pour le Développement (IRD), Université Cheikh Anta Diop de Dakar (UCAD) Hann, Dakar 10700, Senegal; georges.diatta@ird.fr (G.D.); ndiayedame92@gmail.com (D.N.); diagnenafissatou51@gmail.com (N.D.); broaly@live.fr (B.R.T.B.); el-hadj.ba@ird.fr (E.H.B.); diallokalidou3@gmail.com (A.D.); hubert.bassene@ird.fr (H.B.)
2
Departments EMR MINES/UMR MEPHI/RITMES, Campus IHU, Aix-Marseille University, Assistance Publique, Hôpitaux de Marseille (AP HM), Microbes, Évolution, PHylogénie (MEPHI), 19-21 Boulevard Jean Moulin, 13005 Marseille, France; olegusss1@gmail.com (O.M.); alissahhammoud@gmail.com (A.H.)
3
Institut Hospitalo-Universitaire (IHU) Méditerranée Infection, 13005 Marseille, France; sebastien.cortaredona@ird.fr; (S.C.); philippe.parola@univ-amu.fr (P.P.); didier.raoult@gmail.com (D.R.)
4
Institut Pasteur de Paris, 75015 Paris, France; muriel.vray@pasteur.fr
5
Departments EMR MINES/UMR MEPHI/RITMES, Campus IHU, Aix-Marseille University, Assitance Publique, Hôpitaux de Marseille (AP HM), Service de Santé des Armées (SSA), Risques Infectieux, Tropicaux, Microorganismes Émergents (RITMES), 19-21 Boulevard Jean Moulin, 13005 Marseille, France
*
Corresponding author: cheikh.sokhna@ird.fr; Tel.: +221-33849-35-84 or +221-77637-24-99
How to Cite: Diatta, G.; Ndiaye, D.; Diagne, N.; Richmond Tra Bi, B.; Mediannikov, O.; Hammoud, A.; Ba, E.H.; Diallo, A.; Bassene, H.; Vray, M.; et al. Assessment of the Therapeutic Effectiveness of the Combination of Oral Ivermectin and Azithromycin in the Treatment of Head Lice Infestations in Rural Areas of Senegal. Afr. J. Parasitol. Mycol. Entomol. 2026, 4(1): 1; doi:10.35995/ajpme04010001.
Received: 7 October 2025 / Accepted: 15 May 2026 / Published: 22 June 2026
Abstract
:Introduction: Head lice infestations are widespread in Senegal and widely distributed throughout the world with high proportions. Recent studies involving classical treatment modalities and alternative ivermectin treatment indicated the existence of an ivermectin-resistant head lice population. Method: Our study involved oral combination of ivermectin with azithromycin to prevent mutant-resistant lice to treatment with oral ivermectin alone. Each infested participant weighing at last 15 kg was administered orally a single dose of 333 µg/kg of ivermectin combined with one or two 250 mg tablets of azithromycin and/or one 500 mg, repeated on day 7 if lice infestation persisted. Result: Of 315 participants, 308 and 304 patients were respectively followed-up on days 7 and 15, with a respective reduction in infestation of 27.6% and an effectiveness of 66.4% (p ˂ 0.001). On day 28, 280 were no longer infested with lice or living eggs, revealing 96.2% (280/291) effectiveness (p ˂ 0.001) achieved without any participant stopping treatment. Conclusion: After conducting PCR-RFLP assays and sequencing the two mutation sites, no mutation for either polymorphism occurred and no resistant lice were found. Resistant lice subjected to oral ivermectin treatment alone is not likely to be apparent in an infested population treated with oral ivermectin and azithromycin combination.
Keywords:
oral ivermectin and azithromycin combination; head lice treatment; ivermectin resistant lice; rural areas; Senegal1. Introduction
There are two species of lice that can parasitize humans, especially the head louse, Pediculus humanus capitis, which is responsible for pediculosis of the scalp, and the body louse, P. humanus corporis, the agent of human body pediculosis. Every year, more than 100 million people worldwide, largely aged between 3 and 11 years old, are infested with lice [1]. Children remain vulnerable due to their social behaviours (close social and/or physical contact, etc.) which encourage the propagation of parasites within a population. Body lice are involved in the transmission of three bacterial diseases usually encountered in people living in vulnerable sanitary or unfavourable socio-economic conditions, including exanthematic typhus (epidemic) caused by Rickettsia prowazekii, louse-borne relapsing fever due to Borrelia recurrentis, and Bartonella quintana, which causes trench fever and was identified as a major human pathogen during the First World War and caused an epidemic in one million soldiers in Europe [2,3,4,5,6].
For several decades, the treatment of head lice has been based on the use of local insecticide lotions from malathion (0.5% formulation) and permethrin (1% formulation) [7,8]. Such a treatment consists of applying the lotion to the entire hair and must be repeated seven days later, in order to eliminate lice born from nits that were not destroyed during the first treatment [9,10]. Over time, however, many strains of lice have developed resistance to these chemical treatments, which are sometimes toxic and irritating [11]. This resistance means that no treatment is currently effective against certain populations of lice [12]. Insecticides have gradually been competing with alcohol-free products that have no side effects, are more ecological and non-irritating, and are composed of silicone, which immobilize the parasite and suffocate it [7]. However, the effectiveness of these products remains lower than that of a conventional insecticide-based treatment [13,14,15,16,17]. In this context, ivermectin-based products are already used as alternative pediculicides treatments in some countries to combat head lice infestations. Ivermectin (IVER) is an antiparasitic treatment produced by an actinomycete named Streptomyces avermitilis (Fiche DCI VIDAL, 2015). It is currently used in the mass treatment of onchocerciasis, other filariases, and in some intestinal nematodoses as well as in the treatment of scabies and, more rarely, in resistant pediculosis. Recent studies in children have shown good tolerance of oral IVER [18]. Ivermectin was therefore used in oral administration for the treatment of pediculosis [1,19,20]. Azithromycin is the first macrolide antibiotic of the azalide group that acts in synergy with ivermectin. Lice have a bacterium that lives in symbiosis with them, named Candidatus Riesia pediculicola. This bacterium, which provides vitamin B to lice, is necessary for them; however, it can be removed by the synergistic action of the combination of azithromycin and ivermectin [21].
Lice are strictly hematophagous, so when taking a blood meal after ivermectin treatment, there is an inhibitory action on the nerve fibres and muscle cells of the lice through the GABA neurotransmitter, resulting in the death of the lice by paralysis. This treatment kills the nymphs that still reside in living eggs, since the nymphs are also strictly hematophagous from birth. However, living lice are not likely to be removed by ivermectin [19,20,22,23]. The treatment of pediculosis with ivermectin in oral administration makes it possible to remove lice in 95% of cases [1]. However, this treatment may cause lice to become resistant to ivermectin, which can lead to re-infestation. Also, it has been shown that when treating pediculosis with ivermectin alone as an ointment, lice may develop resistance [23,24,25]. Ivermectin-resistant lice exhibit three non-synonymous mutations in the GluCl gene. The A251V (C752T) mutation found in the TM3 transmembrane domain, the S46P (T136C) mutation, is located at the N-terminal extracellular domain and H272R (A815G) is located in the M3-M4 linker transmembrane region of GluCl [26]. The presence of point mutations of the GluCl gene in head lice clinically resistant to ivermectin has recently been reported in the Dielmo population in the Fatick region of Senegal [26]. To overcome the problem of lice resistance to ivermectin, recent in vitro and in vivo studies have shown that the combination of ivermectin and azithromycin presents a synergistic action that has prevented lice resistance and re-infestations associated with treatment using ivermectin alone [27].
In Senegal, B. quintana has been identified in febrile patients in Ndiop, and head lice carriage has a prevalence varying from 5 to 25% depending on age [28,29]. It has also been demonstrated that head lice are probably involved in the transmission of B. quintana [28,30]. A recent study has indicated that there may be a population of head lice which are resistant to ivermectin circulating between women in rural areas [23]. For all these reasons, it seemed necessary to combine the oral administration of ivermectin with azithromycin to boost its action in order to prevent the appearance of mutant resistant lice to treatment with oral ivermectin alone, and to assist practitioners in making therapeutic decisions to fight against head lice infestations within human populations.
2. Materials and Methods
2.1. Study Sites from Health Posts and/or Health Cases
The study was conducted between 16 July and 19 August 2018 in the villages of Dielmo (13º43′ N/16º24′ W), Ndiop (13º41′ N/16º22′ W) (Figure 1), Sabouya (13º43′ N/16º25′ W), Touba-Nding (13º43′ N/16º25′ W), Nema-Nding (13º42′ N/16º25′ W), Medina Santhie (13º42′ N/16º24′ W), and Passy Ndenderling (13º42′ N/16º22′ W) in the Fatick region (Figure 1) of Senegal. These seven villages were divided into five intervention sites (health posts with a nurse and/or health cases with a health worker) as follows:
- Site of Dielmo, Sabouya, Touba-Nding (health post);
- Site of Nema-Nding (health post);
- Site of Medina Santhie (health case);
- Site of Passy Ndenderling (health case);
- Site of Ndiop (health post).
Figure 1.
Map showing location of Dielmo and Ndiop, and the five other surrounding villages, which represent a pragmatic clinical study area, in the Fatick region of Senegal.
Figure 1.
Map showing location of Dielmo and Ndiop, and the five other surrounding villages, which represent a pragmatic clinical study area, in the Fatick region of Senegal.
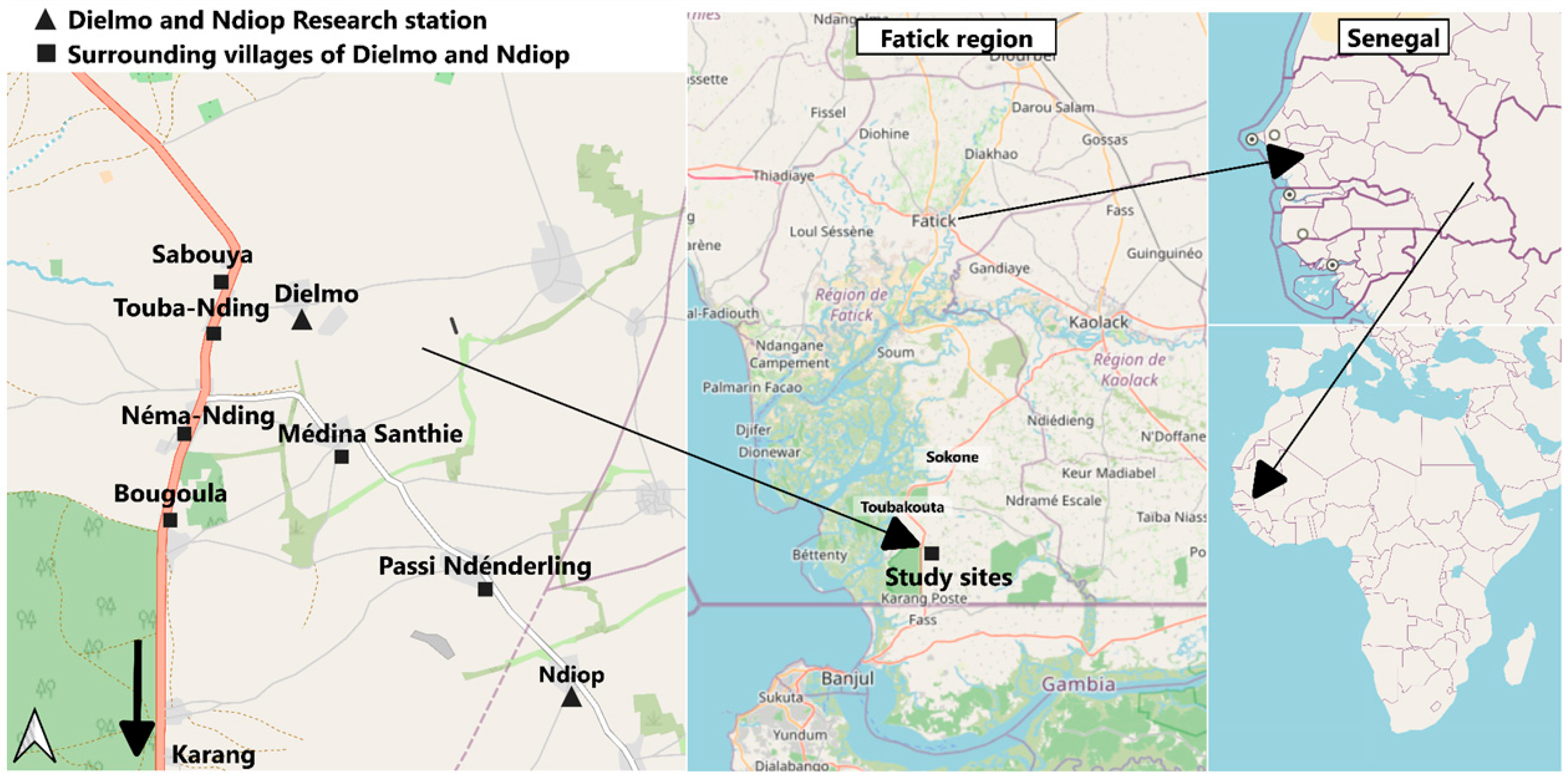
Dielmo and Ndiop are two villages 5 kilometres apart, with the village of Ndiop to the south of Dielmo, which lies 15 kilometres north of the Gambian border. These two villages form the Dielmo and Ndiop Research Station, a collaboration between the French National Research Institute for Sustainable Development (IRD), the Pasteur Institute of Dakar (IPD), and the Ministry of Health and Public Hygiene (MSHP) of Senegal, where parasitological and epidemiological monitoring of the population is regularly conducted 24 hours a day, 7 days a week. To travel from the village of Dielmo to that of Ndiop, one must pass through five other villages, such as Sabouya, Touba-Nding (closest to Dielmo), Néma-Nding, Médina Santhie, and Passy Ndenderling, which we deemed appropriate to include in the pragmatic clinical trial after consulting with each village chief due to the public health significance of head lice infestations. Health posts were located in Dielmo, Néma-Nding, and Ndiop, while health cases existed in Medina Santhie, Passy Ndenderling, and the 5 surrounding villages of Dielmo and Ndiop, thus representing the pragmatic clinical study area (S1: Study protocol).
2.2. Population and Type of Study
The study participants were female children, adolescents, and adults with head lice or nits who met the inclusion and non-inclusion criteria (S1: Study protocol). Boys and men in this community remain not infested. A survey performed four months before the clinical assay revealed a female population of 2066 (S1: Participants checklist) with a prevalence of 22% (454/2066) of head lice infestation, including 11.4% (39/342) in Dielmo, 21.7% (84/387) in Ndiop, 11.8% (11//93) in Sabouya, 9.6% (10/104) in Touba-Nding, 21.2% (124/585) in Nema-Nding, 30.6% (63/206) in Medina Santhie, and 35.2% (123/349) in Passy Ndenderling (S1: Study protocol).
This is a single-arm pragmatic clinical trial to (S1: Study protocol) (i) determine the rate of elimination of head lice and living eggs after the oral administration of oral ivermectin and azithromycin combination on day 7 after the single dose of the drugs, and on days 15 and 28 if the dose is repeated in case of persistent lice or nits; (ii) evaluate the acceptability and clinical tolerance of the AZITH + IVER combination package in the treatment of lice in a single dose; (iii) specify the rate of re-infestation and/or resurgence from living eggs on days 15 and 28 after dosing; (iv) dose the drugs on day 7 and their persistence on days 15 and 28 in the hair after the therapeutic dose; (v) identify the level of selection of resistant lice on days 7, 15, and 28 (in vivo) and specify the mutated genes linked to the resistance of lice to the AZITH/IVER combination; and (vi) assess the effectiveness of the AZITH + IVER combination package on head lice/body lice co-infestations in the same individual, if necessary, in accordance with the hypothesis indicating that oral ivermectin with azithromycin combination package would be more efficient and would avoid the selection of resistant lice to oral treatment with ivermectin alone. Then, the effectiveness of the synergistic action of these two molecules administered in a single dose would efficiently destroy all lice and living eggs with a dose of ivermectin at 333 µg/kg combined with 1 or 2 tablets of 250 mg azithromycin or 1 tablet of 500 mg in a single dose for any body weight greater than or equal to 15 kg (to be repeated on day 7 if lice or nits persist). On day 7, we performed a separate follow-up of participants who had received one dose and were free of lice, and those who received a second therapeutic dose due to the persistence of lice or living eggs. Each participant was recruited on the basis of current head lice or living egg carriage, confirmed after a complete examination of the hair. Three months after the end of enrolment and treatment, post-treatment pruritus research was carried out on day 90, between 26 and 30 November 2018, in order to determine if participants cured with head lice were between-time infested with lice. The timeline details of the clinical study concerning day 0 of the follow-up involved enrolling participants by having them sign an informed consent form and educating them on the precautions to take to prevent infection; day 1 consisted of fasting prior to treatment and post-treatment observation, including a home visit to monitor for any adverse events; days 2, 5, 7, 15, and 28 involved visits to collect dead lice and hair samples taken close to the scalp to assess treatment efficacy, determine the rate of reinfestation and/or recurrence from nits, and evaluate the level of selection of resistant lice on days 7, 15, and 28, and finally on day 90, we assessed for the presence of pruritus following treatment.
2.3. Head Lice and Living Egg Research Strategy
Each participant’s hair was visually checked. Patients infested with head lice or living eggs were carefully examined (S1: Study protocol) by having the patient lean forward with her head between the thighs of a female monitor who attached a white sheet held around her belt plevian (Figure 2A). Since the data collected from the volunteer participants is confidential, their faces in all images have been covered as have those of the female instructors (monitors), in order to protect their privacy (Figure 2A). Appropriate combs and brushes were used (Figure 2B) to untangle and spread the hair to detect lice or living eggs. Lice were sought at usual locations, particularly on either temple and at the nape of the neck. An infestation with lice or nits was confirmed by trained female monitors from each village.
Figure 2.
(A) Female monitors who examined the hair of each participant with an infestation of head lice or living eggs. (B) Appropriate combs and brushes used to untangle the hair of each participant examined.
Figure 2.
(A) Female monitors who examined the hair of each participant with an infestation of head lice or living eggs. (B) Appropriate combs and brushes used to untangle the hair of each participant examined.

2.4. Recruitment and Inclusion of Participants
At each site (health post and/or health case), most participants (S1: Study protocol) attending signed the amended 2018 informed consent form on the eve of the day before the dose administration. Participants who were absent from their homes at the time of the monitors’ visit could come on day 1 to be enrolled at the relevant study site (health post and/or health case). Each enrolled participant with confirmed active infestation of head lice or living eggs (at least 3 live lice or living eggs) as measured by the female monitors, who signed the informed consent form, was assigned a code and all basic information was included in the identification forms. Body weight was also measured at the time of inclusion. All relevant information from each participant was recorded in a case report form (CRF).
It should be noted that inadvertently, the 2017 version of the informed consent form was printed and used instead of the amended 2018 version to collect consent from 107 participants enrolled in two study sites. This error, which was noticed at the end of enrolment in the second site, was brought to the attention of the clinical monitor team as a Contract Research Organization (CRO) and the National Health Research Ethics Committee (CNERS) of Senegal, and we then systematically withdrew these informed consent forms signed by the participants and thus asked the investigators to resume collection of these consents with signatures using the amended 2018 version.
2.5. Inclusion and Non-Inclusion Criteria
Any female infested with head lice or living eggs who had a body weight of 15 kg or more and who gave free consent was included in the study (S1: Study protocol). Infested females weighing less than 15 kg, non-residents of the targeted villages, pregnant or lactating women, and those suspected of being pregnant were not included. However, infested subjects who were not included in the study were nevertheless treated with an anti-louse lotion (brand name “Pouxit”) to avoid contamination or re-infestation (S1: Study protocol).
2.6. Sample Size
The prevalence of head lice infestation identified four months before the pragmatic clinical trial has ranged according to the population of each study site. Consenting participants included in the study were confirmed to have an active head lice or living egg infestation (at least three individuals or living eggs) by four female monitors. Based on the hypothesis of a rate of 98% effectiveness of oral ivermectin and azithromycin combination (head lice removal rate), a delta difference of no more than 15% between participants who were free of head lice at day 28 and those with live head lice or living eggs was necessary, the alpha risk was fixed at 5% to provide a power of more than 95%, and a sample size of 315 female patients was needed (S1: Study protocol). The primary outcome of the study was the pediculicidal effectiveness of therapeutic dose estimated by the rate of disappearance (absence) of head lice on day 7. The secondary outcomes were zero lice at day 7, assuming that oral ivermectin and azithromycin combination is 98% effective [CI 95, 95%–100%], the acceptability and clinical tolerance of the medications by participants, and the absence of head lice or living egg infestation estimated by female monitors on days 15 and 28 when combination therapy is renewed on day 7 if head lice and/or living eggs persist, as well as the absence of genetic selection of resistant lice on days 7, 15, and 28.
2.7. Choose of Already Credible Comparison Control Treatment
Oral ivermectin is an effective treatment for head lice and scabies, and/or at the community level, for onchocercosis through mass drug administration (MDA), although the doses use vary. To interpret easily any difference found during the pragmatic trial using oral ivermectin and azithromycin combination, the oral ivermectin treatment at a dose of 200 µg/kg of body weight administered on days 1 and 8 [31] has been chosen as the reference to measure relative change in head lice prevalence infestation after the intervention.
2.8. Treatment of Enrolled Participants Infested with Head Lice or Living Eggs and Indications for Drugs Administered
Participants included in the study (S1: Study protocol) were admitted on an empty stomach for the IVER + AZITH dose and were observed for one hour after administration of the drugs before being offered a free breakfast. All treatments were given at each site (health post and/or health case) by the team physician and an assistant nurse, and the dosage was based on the body weight related to each participant. The IVER + AZITH dose administered as a single dose based on body weight to each participant was 333 micrograms per kg of oral ivermectin, combined with one or two 250 mg tablets of azithromycin or one 500 mg weighing at last 15 kg, then repeated on day 7 if the lice or living eggs persisted. A cap was systematically worn by each participant after the therapeutic dose had been administered (Figure 3) to contain any dead lice. The number of tablets administered on days 1 and 7 and the occurrence of any adverse events were recorded in a case report form (CRF). Each participant who developed an adverse event after drug treatment was medically managed by the team physician. In addition, to prevent and avoid contamination within the families from which participants were recruited, all ineligible patients infested with head lice or living eggs were treated on day 1 with an anti-louse and living egg lotion (brand name “Pouxit”). These infested patients who were not eligible, but nevertheless treated, were closely monitored on days 1 and 8 until the removal of lice and living eggs.
Figure 3.
Wearing a cap after administration of the therapeutic dose of the ivermectin and azithromycin combination.
Figure 3.
Wearing a cap after administration of the therapeutic dose of the ivermectin and azithromycin combination.

2.9. Measures Taken to Avoid Contamination or Re-Infestation
To prevent the risk of head lice contamination in treated participants by women who were infested and had not previously been identified during the treatment period and follow-up on days 1, 7, 15, and 28, or who had not reported their head lice infestations for social reasons, we considered developing the following strategic measures in the field (S1: Study protocol):
- Mass awareness raising among the populations of the study sites.
- Targeted awareness raising around the need to isolate participants’ beds in families where a female participant was recruited. Mattresses and mosquito nets were made available where necessary.
- Awareness raising to ask each participant to avoid exchanging headscarves and sharing hairdressing material.
2.10. Follow-Up of Study Participants
On each site, the monitors recruited by the project were responsible for (S1: Study protocol):
- Ensuring the follow-up at the home of all participants.
- Collecting and recording on a survey form the occurrence of any adverse events reported on days 1 and 7 in the participants’ homes.
- Installing a white sheet in the evenings of days 1 and 7 on the pillows of each participant for a better view of the dead lice.
- Collecting dead head lice on days 2 and 8 from the participants’ white sheets and caps the day after the treatment.
- Identifying from participants’ live lice at each site on days 7, 15, and 28 when the lice infestation was persistent and collecting 1 or 2 live individuals for genetic analysis.
- Collecting samples from the scalp of each participant on days 2 and 5 at home, and days 7, 15, and 28 at each study site to estimate drug persistence by molecular analysis.
All collected lice and hair were stored at room temperature in Eppendorf tubes marked with the current date and the participant’s code for specific determination and molecular analysis respectively.
2.11. Amplification and Sequencing of GluCl Gene Mutations
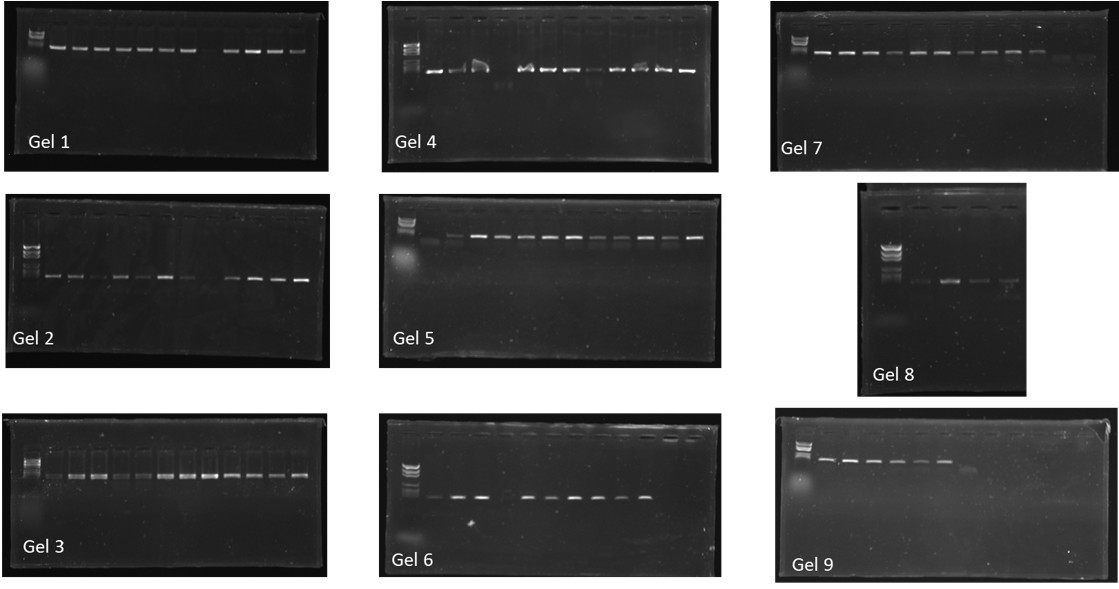
Two sets of primers were used to amplify a 919 bp GluCl gene fragment. Each set of primers amplifies a fragment containing one mutation (Table 1). In brief, PCR was carried out using a Peltier PTC-200 model thermal cycler (MJ Research Inc., Watertown, MA, USA), with a final volume of 25 μL, containing 12.5 μL of Amplitaq gold master mix (Qiagen), 0.75 μL of 10 μM of each primer, 5 μL of DNA template, and nuclease-free water. The standard amplification program was used as follows: one initial denaturation step at 95 °C for 15 min, followed by 39 denaturation cycles of 30 seconds at 95 °C, 30 seconds of annealing at Tm*, and one minute of extension at 72 °C, followed by a final elongation cycle at 72 °C for seven minutes. Finally, in order to determine the success of the reaction, migration on 2% agarose gel was performed and is illustrated as follows:
In preparation for sequencing and RFLP-PCR assay, all the PCR products were purified using NucleoFast 96 PCR plates (Macherey Nagel EURL, Hoerdt, France) following the manufacturer’s instructions. DNA concentration was determined by spectrophotometric quantification through the NanoDrop 1000 (Thermo Fisher Scientific, Waltham, MA, USA). We sequenced a 919 bp and a 547 bp GluCl gene fragment harbouring the H272R (A815G) and A251V (C752T) polymorphisms respectively. Sequencing was performed using the Big Dye Terminator Cycle Sequencing Kit (Perkin Elmer Applied Biosystems, Foster City, CA, USA) with an ABI automated sequencer (Applied Biosystems). The obtained electropherograms were assembled and edited using ChromasPro software (ChromasPro 1.7, Technelysium Pty Ltd., Tewantin, Australia). Prior to the analysis of the nucleotide and mutation sites, a ClustalW multiple alignment was conducted using the BioEdit v 7.0.5.3 software (available online: http://en.bio-soft.net/format/BioEdit.html).

Table 1.
Primer sequences, annealing temperatures, target mutation, and restriction enzymes used for RFLP-PCR and sequencing assay of the GluCl gene.
Table 1.
Primer sequences, annealing temperatures, target mutation, and restriction enzymes used for RFLP-PCR and sequencing assay of the GluCl gene.
| Primer Name | Primer Sequences | Fragment Length | Annealing Temperature | Mutations | Restriction Enzyme |
|---|---|---|---|---|---|
| 6833F | AAGTTGGCGATCCCGTTCAAG | 919 bp | Tm* = 49 °C | H272R (A815G) | HhaI (Cut mutated type) |
| 7750R | CAATCGAATTAATTATCTTCCGT | ||||
| 7203F | GCATCATTGCCACCGGTA | 547 bp | Tm* = 49 °C | A251V (C752T) | NsiI-HF (Cut wild type) |
| 7750R | CAATCGAATTAATTATCTTCCGT |
Tm*: Annealing temperature specific to each set of primers.
2.12. Molecular Diagnostic Assays Based on RFLP-PCR for GluCl Gene Mutation Genotyping
To identify the presence of the H272R (A815G) mutation in the M3–M4 transmembrane linker, a 919 bp fragment was amplified using 6833F and 7750R primers. Successful amplicons were subjected to RFLP analysis using the HhaI (RE) (New England BioLabs, Evry, France) that cuts the 5′...G C G’C... 3′ sequence, therefore detecting a mutated type, resistant to ivermectin. The digestion reaction prepared on ice consisted of a mix of 50 µL containing 5 µL of 1X CutSmart Buffer, 5 µL of 1600 µM S-adenosylmethionine, and 1 µL of 1000 units of HhaI (Methyltransferase) RE, complemented with nuclease-free water. Finally, purified DNA was added with the final concentration of 1 µg. The 50 µL mix was incubated at 37 °C for 60 min followed by an inactivation phase at 65 ºC for 20 min.
Concerning the A251V (C752T) polymorphism, a 547 bp fragment was amplified using 7203F and 7750R primers, and successful amplicons were subjected to RFLP analysis. A mix of 50 µL was prepared on ice, containing 5 µL of 1X NEBuffer and 1 µL of NsiI-HF RE, complemented with nuclease-free water. Finally, purified DNA was added with the final concentration of 1 µg. The 50 µL mix was incubated at 37 °C for 60 min followed by the addition of 10 µL of 6X gel loading dye to stop the reaction. The NsiI-HF RE (New England BioLabs) cuts the 5′...A T G C A’T... 3′ sequence, therefore detecting a wild type, susceptible to ivermectin. The digested PCR products were separated on 3% agarose gel.
2.13. Statistical Analysis
The absence and/or presence of head lice or living eggs (none or one head louse and/or living egg) after treatment was estimated on days 7, 15, and 28 by four female monitors in order to assess the effectiveness of oral ivermectin and azithromycin combination. The variation in the proportions of infestation by age group, and of the therapeutic effectiveness of oral ivermectin and azithromycin combination at days 7, 15, and 28, and then between study sites and by age group were evaluated. To compare the therapeutic effectiveness variables of the dose administered on days 7, 15, and 28, then between study sites and age groups, Chi-squared tests were applied. Analyses involved two sided p-values, with statistical significance defined by p < 0.05. Excel (version 2010) software was used for data entry and descriptive analysis. Statistical tests were performed using OpenEpi Version 3.01 updated on 6 April 2013 [32].
3. Results
3.1. Criteria for Judging Therapeutic Effectiveness
The first endpoint for pediculicidal effectiveness was estimated by the absence of head lice or living eggs on day 7. The absence of head lice and living eggs on day 7 was determined by five monitors combing one after the other until no live lice or living eggs were found on the entire scalp of each participant examined. The clinical acceptability, tolerance of drugs, and residual effects (persistence) of administered medications in participants was also a good indicator of effectiveness. The absence of lice or living eggs on days 15 and 28 obtained following the repetition of the therapeutic dose IVER + AZITH on day 7 due to the persistence of lice or living eggs is an equally important indicator. The counting of dead lice individuals on each participant’s white sleeping sheet or cap on days 2 and 8 was a good marker of effectiveness, as was the absence of resistant lice on days 7, 15, and 28.
3.2. Prevalence of Pediculosis Among Participants and by Age Group
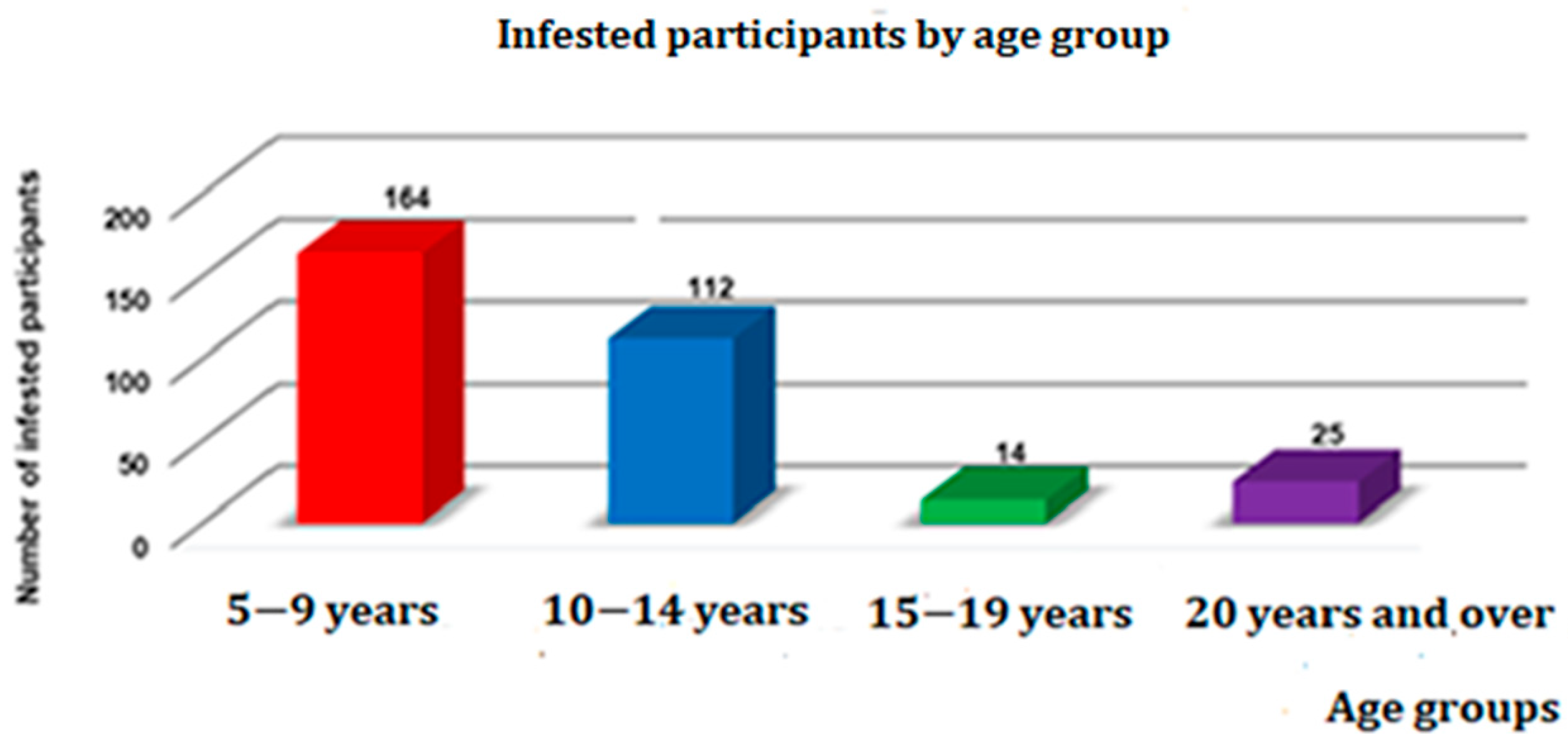
The overall prevalence of head lice infestations in the study area was 15.2% (315/2066). This varied according to the population of women at each site, and represented 6.7% (23/342) in Dielmo, 5.1% (10/197) in Sabouya and Touba-Nding, 12.6% (74/585) in Nema-Nding, 20.8% (43/206) in Medina Santhie, 27.8% (97/349) in Passy Ndenderling, and 17.6% (68/387) in Ndiop. The group between the ages of 5 and 9 was the most infested, with 52% (164/315), followed by the 10–14 age group with 35.5% (112/315), the over 20 age group with 7.9% (25/315), and the 15–19 age group with 4.4% (14/315) (Figure 4). There was a significant variation in the prevalence of head lice infestation between age groups (p = 0.008).
Figure 4.
Prevalence of head lice infestation among participants by age group (n = 315).
3.3. Participants and Baseline Study Data
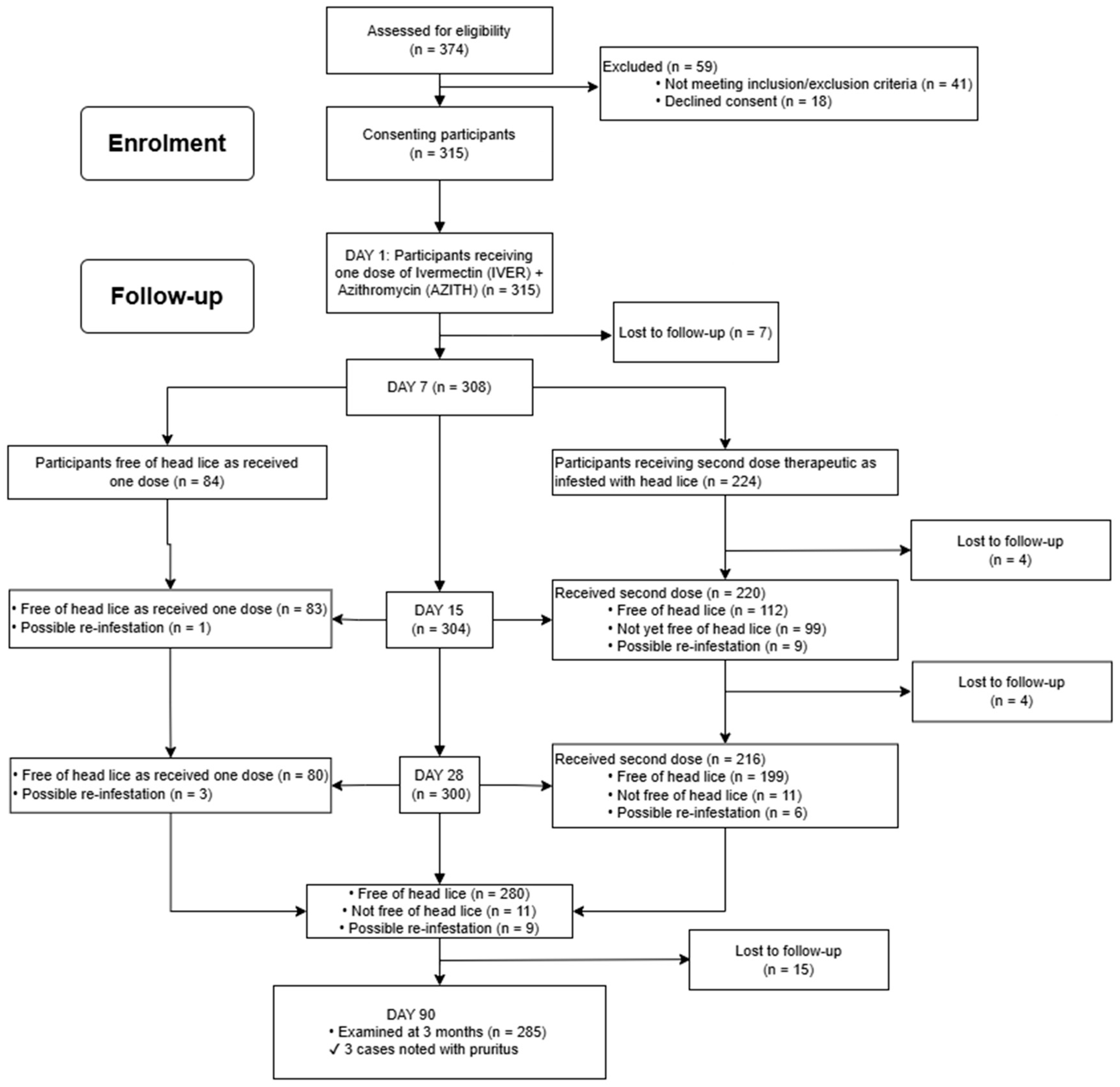
The process of enrolling and following-up with participants through the clinical trial is presented in Figure 5. Of the 374 eligible subjects, 315 participants signed the informed consent form and were enrolled, screened for head lice infestations, and received orally on day 1 one dose of ivermectin and azithromycin combination. On day 7, seven patients from the group receiving the first dose were lost to follow-up. Of 308 participants evaluated on day 7, 84 who had received one dose were free of head lice and 224 who were still infested with head lice received the second therapeutic dose. On day 15, out of 224 cases evaluated, four patients were lost to follow-up, 112 were free of head lice, 99 were not yet free of their lice infestation, and nine cases of probable lice re-infestation were found, including one case of probable lice re-infestation in the group receiving one dose. On day 28, three cases of probable lice re-infestation were noted in the group receiving one dose, and in the group who had been given the second dose, there were four patients lost to follow-up at the time of the control, 200 were free of head lice, 11 were not yet lice-free, and there were six cases of probable lice re-infestation. In total, there were 280 participants who were free of head lice, 11 with live head lice, and 11 cases of probable lice contamination. On day 90, out of 300 participants of the group regularly monitored until day 28, there were 15 patients lost to follow-up at the time of the control, and 285 participants were examined without finding louse infestation, but three cases of pruritus were noted.
Figure 5.
Enrolment and follow-up flowchart for pragmatic clinical study participants, in Senegal, July–August 2018.
Figure 5.
Enrolment and follow-up flowchart for pragmatic clinical study participants, in Senegal, July–August 2018.
3.4. Assessment of the Therapeutic Effectiveness of the Drugs Administered
Evaluation of the therapeutic effectiveness of the combination of oral ivermectin and azithromycin showed that on day 7 after the first treatment, 224 participants (72.7%) had live head lice and 84 were cured with a reduction in their lice infestation of 27.3% (84/308). On day 15 after the second treatment, 11 participants (3.5%) were lost to follow-up at the time of the control (Table 2), and 196 patients were free of lice with therapeutic effectiveness of 66.4% (196/295), compared to 99 (33.6%, 99/295) who continued to have live lice and/or living eggs (Table 2). There was a significant variation in the rate of cure of head lice infestation in participants between days 7 and 15 (p < 0.001). On day 28 post-treatment, 280 patients were completely cured of their lice with a high effectiveness of 96.2% (280/291), and only 11 participants (3.8%, 11/291) still had live head lice, with nine cases of lice possible re-infestation identified and 15 people who were lost to follow-up at the time of the control (Table 2). A significant difference in treatment effectiveness was noted at days 15 and 28 (p < 0.001), with a significant variation in the therapeutic effectiveness of oral ivermectin and azithromycin combination at days 7, 15, and 28 (p < 0.001). (Table 2). The change in proportion of participants that were found cured of their lice ranged significantly between study sites at day 7 (Table 3 and Table 4) (p = 0.014), while at days 15 and 28, this variation in proportion of patients free of their head lice was not significant between study sites (Table 3 and Table 4) (p = 0.678 and p = 0.999 respectively). In addition, variation in treatment effectiveness between age groups was significant at days 7 and 15 (p = 0.001), as well as at days 7 and 28 (p = 0.036), and non-significant, however, at days 15 and 28 (p = 0.109).
Table 2.
Evaluation of treatment effectiveness of oral ivermectin and azithromycin combination on days 7, 15, and 28 post-treatment, July–August 2018 (n = 315).
Table 2.
Evaluation of treatment effectiveness of oral ivermectin and azithromycin combination on days 7, 15, and 28 post-treatment, July–August 2018 (n = 315).
| Treatment Effectiveness | |||
|---|---|---|---|
| At Day 7 | At Day 15 | At Day 28 | |
| Control Type from Followed-Up Participants Processed | Status of Participants Processed | Status of Participants Processed | Status of Participants Processed |
| Participants free of head lice | 84 (27.3%) | 196 (66.4%) | 280 (96.2%) |
| Participants not free of head lice | 224 (72.7%) | 99 (33.6%) | 11 (3.8%) |
| Participants lost to follow-up | 7 (2.3%) | 11 (3.6) | 15 (4.8%) |
| Possible re-infestation | 0 | 9 (2.9%) | 9 (3%) |
| * p-value | * p ˂ 0.001 | * p ˂ 0.001 | |
| Total | 315 | 315 | 315 |
* = Significant variation in the therapeutic effectiveness of oral ivermectin and azithromycin combination at days 7, 15, and 28.
Table 3.
Therapeutic effectiveness of oral ivermectin and azithromycin combination evaluated by study site and overall on days 7 and 15 post-treatment, in July–August 2018 (n = 315).
Table 3.
Therapeutic effectiveness of oral ivermectin and azithromycin combination evaluated by study site and overall on days 7 and 15 post-treatment, in July–August 2018 (n = 315).
| Villages Studied | Enrolled Participants | Lost to Follow-Up at Day 7 | Number of Participants at Day 7 | Lost to Follow-Up at Day 7–Day 15 | Number of Participants at Day 7–Day 15 | Negative at Day 7 | Positive at Day 7 | Negative at Day 15 | Positive at Day 15 | Probable Cases of Contamination (Re-Infestation) at Day 15 |
|---|---|---|---|---|---|---|---|---|---|---|
| Dielmo, Sabouya, Touba-Nding | 33 | 4 | 29 | 5 | 28 | 11 (39.3%) | 18 (62%) | 22 (78.6%) | 6 (21.4%) | Nothing to report |
| Nema-Nding | 74 | 0 | 74 | 1 | 73 | 27 (37%) | 47 (63.5%) | 47 (66.2%) | 24 (33.8%) | 2 (3.6%) cases sometimes sleeping in the bed of an untreated infested mother |
| Medina Santhie | 43 | 1 | 42 | 1 | 42 | 9 (21.4%) | 33 (78.6%) | 28 (66.6%) | 14 (33.3%) | Nothing to report |
| Passy Ndenderling | 97 | 2 | 95 | 2 | 95 | 28 (29.5%) | 67 (70.5%) | 60 (63.2%) | 35 (36.8%) | Nothing to report |
| Ndiop | 68 | 0 | 68 | 2 | 66 | 9 (13.6%) | 59 (86.7%) | 39 (66.1%) | 20 (3.9%) | 7 (10.6%) cases including 3 and 4 others who slept with untreated infested sisters and mothers respectively |
| Total | 315 | 7 (2.3%) | 308 (97.7%) | 11 (3.6%) | 304 (96.5%) | 84 (27.3%) | 224 (72.7%) | 196 (66.4%) | 99 (33.6%) | 9 (2.9%) |
Table 4.
Therapeutic effectiveness of oral ivermectin and azithromycin combination evaluated by study site and overall on days 7, 15, and 28 post-treatment, in July–August 2018 (n=315).
Table 4.
Therapeutic effectiveness of oral ivermectin and azithromycin combination evaluated by study site and overall on days 7, 15, and 28 post-treatment, in July–August 2018 (n=315).
| Villages Studied | Enrolled Participants | Lost to Follow-Up at Day 28 | Number of Participants at Day 28 | Negative at Day 7 | Positive at Day 7 | Negative at Day 15 | Positive at Day 15 | Negative at Day 28 | Positive at Day 28 | Probable Cases Of Contamination (Re-Infestation) at Day 15 | Probable Cases of Contamination (Re-Infestation) at Day 28 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dielmo, Sabouya, Touba-Nding | 33 | 5 | 28 | 11 (39.3%) | 18 (60.7%) | 22 (78.6%) | 6 (21.1%) | 27 (100%) | 0 | Nothing to report | 1 (3.6%) case sometimes sleeping in the bed of an untreated infested mother |
| Nema-Nding | 74 | 1 | 73 | 27 (37%) | 47 (63%) | 47 (66.2%) | 24 (33.8%) | 68 (95.8%) | 3 (4.2%) | 2 (2.7%) Cases sometimes sleeping in the bed of an untreated infested mother | 2 (2.7%) cases sleeping in the bed of their untreated infested sister |
| Medina Santhie | 43 | 1 | 42 | 9 (21.4%) | 33 (78.6%) | 28 (66.6%) | 14 (33.3%) | 39 (92.8%) | 3 (7.1%) | Nothing to report | Nothing to report |
| Passy Ndenderling | 97 | 3 | 94 | 28 (29.5%) | 67 (70.5%) | 60 (63.2%) | 35 (36.8%) | 89 (95.7%) | 4 (4.3%) | Nothing to report | 1 (1.1%) case sleeping with her breastfeeding child who was infested and untreated |
| Ndiop | 68 | 5 | 63 | 9 (13.6%) | 59 (86.4%) | 39 (66.1%) | 20 (33.9%) | 57 (98.3%) | 1 (1.7%) | 7 (10.6%) Cases including 3 and 4 others who slept with untreated infested sisters and mothers respectively | 5 (7.9%) cases including 3 and 2 others who slept with untreated infested sisters and mothers respectively |
| Total | 315 | 15 (4.8%) | 300 (95.2%) | 84 (27.3%) | 224 (72.7%) | 196 (66.4%) | 99 (33.6%) | 280 (96.2%) | 11 (3.8%) | 9 (2.9%) | 9 (3%) |
3.5. Assessment of the Acceptability and Clinical Tolerance of Drugs
A standard operating procedure according to the indications of the drug manufacturer was available, which allowed the medical team (physician and nurse) to administer the dose appropriately. None of the enrolled participants vomited within 30 min of the dose being administered nor within 30 to 60 min after administration, giving a drug acceptability of 100%. In contrast, 278 (88.2%) of the 315 treated participants perfectly tolerated the drugs administered, while 37 others (11.7%) developed adverse events at home on day 1 related to the administration of the therapeutic dose, including dizziness in 19 cases, headache in eight cases, fatigue in eight cases, nausea in six cases, and vomiting with abdominal pain in five cases. Four patients developed both headache and dizziness and another developed nausea and dizziness. One participant reported signs of headache, vertigo, and fatigue. The most frequently reported clinical sign was vertigo (51.6%). Participants who developed adverse events were visited by the physician who administered outpatient treatment with 500 mg of metronidazole in adults or 250 ml in children, an antibiotic and antiparasitic drug best known by its brand name Flagyl, indicated for the treatment of anaerobic bacterial infections, bacterial vaginosis, trichomoniasis, amoebiasis (intestinal/hepatic), giardiasis, and certain dental infections, and either 500 mg of paracetamol in adults or 60 mg/kg or vogalene syrup in children to relieve these pains. Medical rest and sufficient drinking water was advised for clinical signs related to dizziness and fatigue.
3.6. Assessment of Contamination or Re-Infestation Rates on Days 15 and 28
Any infestation of persistent head lice identified on day 15 or 28 which was related to sharing bedding, scarves, and/or hairdressing items with an untreated infested female was considered as probable contamination or re-infestation. Of 304 participants followed regularly until day 15, nine cases of contamination (2.9%) were observed (Table 3), including two cases (2.7%, 2/73) at the Nema-Nding site and seven others (10.6%, 7/66) at the Ndiop site. In contrast, on day 28, out of 300 patients followed, nine cases (3%) of re-infestation were noted (Table 4), including one case (3.6%, 1/28) at the Dielmo, Sabouya, and Touba-Nding site, two cases (2.7%, 2/73) at Nema-Nding, one case (1.1%, 1/94) at Passy Ndenderling, and five other cases (7.9%, 5/93) at Ndiop. No cases of contamination were identified at the Medina Santhie site.
3.7. Identification of GluCl Gene Mutations Related to Head Lice Resistance to Oral Ivermectin
RFLP-PCR assays were used to genotype individual head lice collected in Senegal after the administration of oral ivermectin and azithromycin combination. In total, 34 samples were subjected to the amplification of the GluCl fragment containing the A251V (C752T) and H272R (A815G) polymorphism followed by the application of NsiI-HF and HhaI RE. The amplification of a 547 bp fragment harbouring the A251V (C752T) polymorphism using 7203F and 7750R primers was successful in 24/34 of tested specimens. Following the application of the NsiI-HF RE cutting the 5′...ATGCA’T... 3′ site, migration of the amplicons on 3% agarose gel revealed the presence of three bands with a 547 bp, 440 bp and 107 bp length, which is the expected endonuclease activity described in the study conducted previously [14]. The NsiI-HF restriction site is present on the wild type GluCl sequence, considering that all of our samples presented an endonuclease reaction targeting two sites, thus generating three bands; these results correspond to the presence of a heterozygote polymorphism in our 24 lice specimens (5′...ATGCA’T... 3′ wild susceptible type) (5′...ATGTAT... 3′ mutated resistant type). The 919 bp fragment of the GluCl gene containing the H272R (A815G) polymorphism was amplified using 6833F and 7750R primers in 20/34 of tested lice specimens. Following that, we applied the HhaI RE that cuts the 5′... GCG’C... 3′ site. Migration of the amplicons on 3% agarose gel revealed the presence of one 919 bp band corresponding to the absence of any endonuclease activity. The HhaI RE restriction site is present on the mutated type GluCl sequence, considering that all of our samples showed the absence of a dual agarose band profile; we can confirm the absence of any ivermectin resistant polymorphism in our 20 lice specimens (5′... ACGC... 3′ wild susceptible type) (5′... GCG’C... 3′ mutated resistant type) (Figure 6).
Figure 6.
PCR-RFLP assay for genotyping H272R and A251V mutations of the GluCl gene on head lice collected in Dielmo-Ndiop and surrounding villages, in the Fatick region of Senegal, July–August 2018: (A) 1722 bp fragment of the GluCl gene, exhibiting seven exons and six introns. The sixth exon presents the two RE recognition sites. (B) NsiI-RE site, ATGCA’T, located on the wild type sequence and HhaI-RE site, GCG’C, located on the mutated type sequence. (C) SYBR safe-stained 3% agarose gels showing the DNA fragments’ migration after digestion with NsiI and HhaI RE. –: site of RE endonuclease activity. (D) Alignment of reference sequence (GenBank accession N. DS235786.1) of the GluCl gene fragment with the resistant polymorphisms and with the sequences obtained from head lice collected in Dielmo and Ndiop and surrounding villages, in the Fatick region of Senegal, July–August 2018. Restriction sites of the NsiI and HhaI RE are shown on each sequence. RS: restriction site. HL: head lice.
Figure 6.
PCR-RFLP assay for genotyping H272R and A251V mutations of the GluCl gene on head lice collected in Dielmo-Ndiop and surrounding villages, in the Fatick region of Senegal, July–August 2018: (A) 1722 bp fragment of the GluCl gene, exhibiting seven exons and six introns. The sixth exon presents the two RE recognition sites. (B) NsiI-RE site, ATGCA’T, located on the wild type sequence and HhaI-RE site, GCG’C, located on the mutated type sequence. (C) SYBR safe-stained 3% agarose gels showing the DNA fragments’ migration after digestion with NsiI and HhaI RE. –: site of RE endonuclease activity. (D) Alignment of reference sequence (GenBank accession N. DS235786.1) of the GluCl gene fragment with the resistant polymorphisms and with the sequences obtained from head lice collected in Dielmo and Ndiop and surrounding villages, in the Fatick region of Senegal, July–August 2018. Restriction sites of the NsiI and HhaI RE are shown on each sequence. RS: restriction site. HL: head lice.
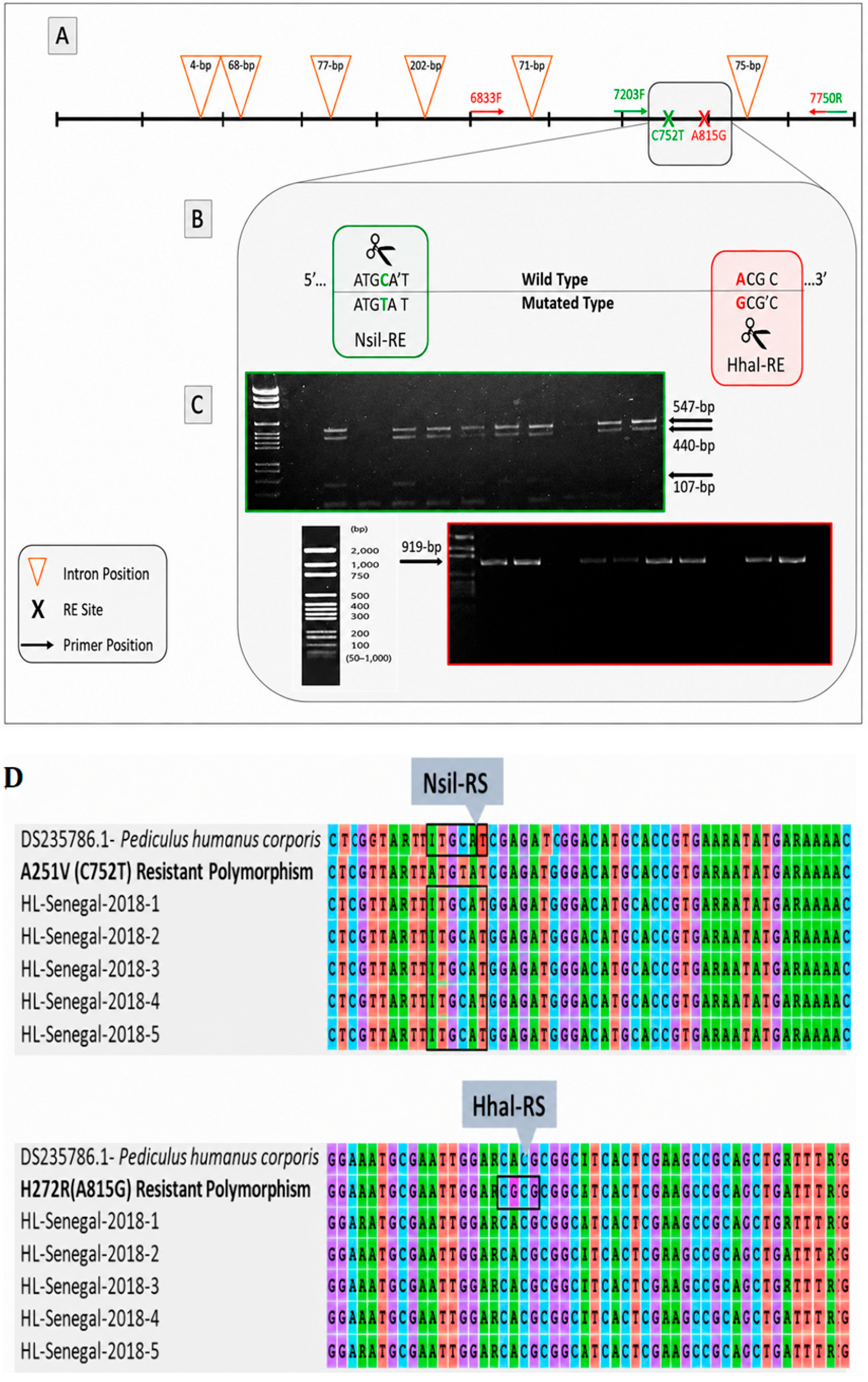
Furthermore, sequencing of these two mutation sites was performed in 30/34 head lice DNA samples, collected from 19 patients. We were able to generate a 960 bp sequence for all selected specimens; 19/30 of the GluCl fragment gene sequence were from specimens collected on day 28 post-treatment and 9/30 were collected on day 2, while only 2/30 sequences were from lice specimens removed on day 7. The alignment of all sequences showed the absence of the heterozygote A251V (C752T) polymorphism and the H272R (A815G) polymorphism, both responsible for resistance to ivermectin (Figure 6D). This result suggests that none of these lice specimens are resistant to oral ivermectin and azithromycin combination.
3.8. Assessment of the Occurrence of Pruritus After Treatment on Day 90
The post-treatment examination for researching pruritus and louse infestation was performed on day 90 in 300 participants regularly followed from day 1 to day 28. Of these 300 participants, 15 (5%) were lost to follow-up at the time of the examination, including four (5.5%, 4/73) in Nema-Nding, three (7.1%, 3/42) in Medina Santhie, three (3.2%, 3/94) in Passy Ndenderling, and five (7.9%, 5/63) in Ndiop. Out of 285 participants examined, no case of louse infestation was identified, while three cases (1%) of pruritus were noted (Figure 7), including two cases (5.1%, 2/39) in Medina Santhie and one (1.7%, 1/58) in Ndiop.
Figure 7.
Case of pruritus observed on day 90 in a participant regularly followed-up with during the clinical study from day 1 to day 28 post-treatment.
Figure 7.
Case of pruritus observed on day 90 in a participant regularly followed-up with during the clinical study from day 1 to day 28 post-treatment.

4. Discussion
In our pragmatic clinical study, ongoing policy actions coupled with an appropriate research approach were used and made the results robust, whilst acknowledging any inherent limitations. This is the first pragmatic clinical trial in a community to demonstrate therapeutic effectiveness based on oral ivermectin and azithromycin combination to treat head lice infestations using ivermectin (333 micrograms per kg) combined with one or two 250 mg tablets of azithromycin and/or one 500 mg in a single dose for any body weight greater than or equal to 15 kg, repeated on day 7 in the event of persistent live lice or living eggs. The clinical acceptability and tolerance of drugs by participants obtained during this study were a good indicator of effectiveness. The absence of head lice and living eggs on days 15 and 28 observed following the repetition of the therapeutic dose IVER + AZITH on day 7 due to the persistence of lice or living eggs was an equally important indicator. Likewise, the counting of dead lice individuals on each participant’s white sleeping sheet or cap on days 2 and 8 was a good marker of effectiveness, as well as the absence of resistant lice on days 7, 15, and 28. At the beginning of the study, among 374 (18.1%) of 2,066 eligible subjects, 315 (15.2%) infested participants signed the informed consent form. This prevalence varied from 5.1% to 27.8% according to the population of women at each site, and the age group between 5 and 9 years was the most infested with 52% (164/315), followed by the 10–14 age group with 35.5% (112/315) as previously reported by Coscione et al. [31], and the over 20 age group (7.9%, 25/315). Children remain vulnerable because of their social behaviours (games, etc.), which is the source of propagation of lice parasites within a population. The boys and men were not found to be infested with head lice, which is why they were not enlisted in our study. This could be explained by the fact that in Sub-Saharan Africa, particularly in Senegal, boys and men who might be found infested with head lice are systematically shaved of their hair, which is rare in women and is even considered inappropriate within the female community. Previous studies in Dielmo and Ndiop women populations indicated a head lice infestation rate of 34.8% and 60.7%, respectively, prior to treatment [20].
The therapeutic dose of the drugs administered (oral ivermectin + azithromycin combination) revealed a high effectiveness (96.2%, 280/291), which was achieved at day 28 post-treatment without any participants stopping treatment due to adverse events. There is a significant variation in the therapeutic effectiveness of oral ivermectin and azithromycin combination on days 7, 15, and 28. On day 15 post-treatment, the dose effectiveness of the drugs administered (oral ivermectin and azithromycin combination) was average (66.4%, 196/295), while on day 7, the dose effectiveness appeared low (27.6%, 84/304). In two studies performed on European and Melanesian patients, an equivalent high effectiveness of 95.2% and 89.1% was reached respectively on day 15 and two-weeks post-treatment with respective oral doses of 400 and 200 micrograms per kg of ivermectin [1,31]. On day 28 post-treatment, the therapeutic effectiveness of oral ivermectin and azithromycin combination was high (96.2%), which may be explained by the high persistence of these drugs and probably to the hair texture of black participants. It is relevant to consider the difference in hair texture between black and white people, which is related to the capillary dynamics of blood flow to the hair, since in two studies of treatment of head lice infestations in European and Melanesian patients, the therapeutic effectiveness equivalent (95.2% and 89.1%) [19,33] to that of our pragmatic clinical study for each of these treatments using oral ivermectin was reached on day 15 and at two-weeks post-treatment. Moreover, in a recent study performed in the village of Dielmo in the Fatick region of Senegal, the effectiveness of the treatment against head lice was 77.4% [20] on day 15 post-treatment in the group receiving oral ivermectin. This result seems to confirm our hypothesis, which we believe to be associated with the texture of black hair that could impact the kinetics of ivermectin action by the capillary route to reach lice or living eggs in the hair. This pragmatic trial study showed the persistence of live head lice (3.8%), which could be explained by the probable hatching of living eggs of which N1, N2, and/or N3 stage nymphs did not take a blood meal that would have brought them into contact with the therapeutic dose of the drugs.
It is notable that the acceptability of oral administration of the drugs within participants tested was 100%, although all adverse events reported in this pragmatic clinical study, such as dizziness, headache with fatigue, nausea, and vomiting with abdominal pain, appear to be secondary. Usually, the clinical tolerance of a drug depends on its pharmacodynamics and pharmacokinetics and is specifically tolerated according to the biological and biochemical constitution of each infested participant. In any case, it may be necessary for the pharmaceutical laboratory manufacturing the combination of ivermectin and azithromycin to perform blood tests on patients who had developed adverse events related to the administration of the dose recommended in order to better understand the biological and biochemical parameters that cause these observed minor adverse events, which were reported in only a few treated participants. Oral administration of the therapeutic dose of ivermectin and azithromycin combination repeated when head live lice or living eggs persisted showed that all participants fully accepted the drugs administered without vomiting after one hour. However, clinical tolerance of the dose administered was 88% in participants, while 12% developed minor adverse events that are likely to be related to the administration of the dose. In 3.8% (11/291) of participants, live head lice were identified and nine cases of contamination were noted.
All head lice that were tested by molecular biology targeting the GluCl fragment containing the H272R (A815G) polymorphism harboured no mutation at this site. While targeting the most prevalent A251V (C752T) site located at the TM3 transmembrane domain, known to be important in the chloride channel pore formation, reducing ivermectin sensitivity [34], PCR-RFLP results showed the presence of a heterozygote polymorphism that was not confirmed by sequencing. We believe that PCR-RFLP is a more sensitive molecular tool for the identification of heterozygote polymorphisms. The multiple attempts to amplify the 865 bp fragment containing the S46P (T136C) polymorphism were unsuccessful using primers described in the study conducted by Amanzougaghene et al. [26]; the attachment site of the primers is located on the intron region of the GluCl gene, which could influence the amplification success. In addition, 19/30 of the generated DNA sequences were from specimens collected at day 28 post-treatment and none of these specimens developed a resistant profile to the combined ivermectin and azithromycin treatment. However, it is still not known whether these mutations contribute directly to ligand binding, or whether they cause conformational changes that influence ligand binding [26]. Molecular biology analyses by sequencing and RFLP-PCR assays were used to genotype collected head lice, and all lice tested showed no mutations on the GluCl fragment and did not identify any polymorphism resistant to the ivermectin and azithromycin combination. These genetic analyses appear to confirm previous in vitro and in vivo work [29], which stated that azithromycin acts synergistically to boost the action of ivermectin and can reduce or prevent the development of resistance in lice by being more effective than current treatments. Head lice resistance to ivermectin, already suspected in 2016 in the population of Dielmo [23] in the Fatick region of Senegal, and confirmed in 2018 by work that identified the presence of mutations in the GluCl gene associated with ivermectin-resistant head lice [26], is not likely to be apparent in an infested population treated with the therapeutic oral dose of the ivermectin and azithromycin combination.
In view of the highly interesting results obtained from this pragmatic clinical study, we strongly believe that as the methodological approach and design of the study appear to be replicable interventions in head lice-infested populations should be conducted in the future on a larger scale to assess the practical value of the oral combination of ivermectin and azithromycin in the treatment of pediculosis and to provide recommendations to the pharmaceutical company to help them make decisions regarding the formulation of the package “ivermectin and azithromycin” in the treatment of pediculosis. The appearance of post-treatment pruritus in a lice-free patient is a marker that reveals conclusive contact with a person and/or tools infested with head lice in the 90 days following the end of the treatment, which would suggest a starting and/or an imminent pediculosis in sight.
Some limitations of our pragmatic clinical trial may be related to the fact that no biochemical analysis of participants’ blood samples was performed before and after administration of the therapeutic dose to assess the identified adverse events and to ensure that they were specifically related to either the medication drugs or a chronic pathology of the participant. Furthermore, the fact that only head lice-infested females participated in this study seems to wrongly indicate a limitation, which we do not believe to be the case, since boys and men were not infested due to the societal context that we explained earlier in the discussion and strongly justifies that the encouraging results of this study can be applied to an intervention extended to the general population.
In conclusion, it appears that this pragmatic clinical trial was conducted with a single arm and was unblended; however, a significant success rate (96.2%, 280/291) was achieved, demonstrating that the combination of ivermectin with at least one antibiotic compound, such as azithromycin, increases the synergistic action to avoid and/or prevent head lice resistance. The therapeutic dose of the combination of ivermectin and azithromycin administered per os in line with the methods employed in our study appears promising for pediculosis eradication within endemic and at-risk communities. These results will certainly make a major, useful contribution to the health, academic, and pharmaceutical knowledge base in the treatment of pediculosis in schools and endemic communities.
Supplementary Materials
The following are available online at https://ajpme.jams.pub/conversion/supplementary/f1fc64e655317d12164b8fa8d585d5ca. S1: Study protocol. S1: Participants checklist.
Author Contributions
Conceptualization: G.D., N.D., B.R.T.B., and E.H.B.; Data curation: G.D. and N.D.; Formal analysis: G.D., N.D., B.R.T.B., J.-M.R., P.P., and D.R.; Funding acquisition: C.S.; Investigation: G.D., D.N., N.D., B.R.T.B., O.M., A.H., A.D., E.H.B., and H.B.; Methodology: G.D., N.D., D.N., B.R.T.B., A.D., E.H.B., H.B., S.C., P.P., J.-M.R., D.R., O.M., and C.S.; Software: G.D., N.D., and B.R.T.B.; Supervision: G.D., N.D., and B.R.T.B.; Validation: G.D., N.D., B.R.T.B., A.D., S.C., J.-M.R., P.P., D.R., and C.S.; Visualization: G.D., N.D., D.N., B.R.T.B., S.C., J.-M.R., P.P., O.M., D.R., and C.S.; Writing—original draft: G.D.; Writing—review and editing: G.D., N.D., D.N., B.R.T.B., E.H.B., A.D., A.H., H.B., M.V., J.-M.R., P.P., D.R., O.M., and C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This pragmatic clinical study was funded by the company Arthrobac Pharma, with Grant number 6020A1. The authors received no specific funding for this work. However, one of the authors (DR) was among the founders of the simplified joint-stock company Arthrobac Pharma for the research and development of products to treat pediculosis. This company now closed.
Institutional Review Board Statement
The pragmatic clinical study was conducted in accordance with the Good Clinical Practice Guidelines of the International Conference on Harmonisation, and the authors declare that the investigations were carried out following the rules of the Declaration of Helsinki of 1975 and its amendments. The protocol for this study was reviewed and approved by the National Committee of Ethics for Health Research (CNERS), then authorized by the Directorate of Planning, Research and Statistics (DPRS) of the Ministry of Health and Social Action of Senegal, reference SEN 16/17, under statement number #0071/MSAS/DPRS/CNERS in 22 June 2017, and another statement number #0045/MSAS/DPRS/CNERS on 22 June 2018 for the request to amend the referenced protocol. Written consent was obtained from all participants by a staff member fluent in local languages (Serere and/or Ouolof). Parents or guardians provided written consent for participants aged below 18 years. In addition, the study project was approved by the Consultative Committee for Ethics and Professional Conduct (CCDE) of the Institute of Research for Development (IRD), France, on 28 February 2018, and then prospectively registered on ClinicalTrials.gov, NCT03578679.
Data Availability Statement
The data supporting reported results can be found on the server of the Research Unit on Infectious, Neglected and Emerging Diseases in the South (MINES) of the Institute of Research for Development (IRD) in Dakar, under to the publicly access link for archived datasets analyzed or generated: https://dataverse.ird.fr/dataset.xhtml?persistentId=doi:10.23708/IWTQZV&version=DRAFT.
Acknowledgments
We are grateful to the populations of the villages we studied for their participation. Our thanks also go to the investigators and medical team who executed this detailed clinical study. The pragmatic clinical trial was supervised by Pharmalys Ltd., a clinical monitor team as a Contract Research Organization (CRO), based in Dakar, Senegal.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in this pragmatic clinical study design; the collection, analysis or interpretation of data; in the decision to publish the results; or the writing of the manuscript.
References
- Chosidow, O.; Giraudeau, B.; Cottrell, J.; Izri, A.; Hofmann, R.; Mann, S.G.; Burgess, I. Oral Ivermectin versus Malathion Lotion for Difficult-to-Treat Head Lice. N. Engl. J. Med. 2010, 362, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Brouqui, P. Arthropod-Borne Diseases Associated with Political and Social Disorder. Annu. Rev. Entomol. 2011, 56, 357–374. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Matthaiou, D.K.; Rafailidis, P.I.; Panos, G.; Pappas, G. Worldwide Prevalence of Head Lice. Emerg. Infect. Dis. 2008, 14, 1493–1494. [Google Scholar] [CrossRef] [PubMed]
- Raoult, D.; Roux, V. The Body Louse as a Vector of Reemerging Human Diseases. Clin. Infect. Dis. 1999, 29, 888–911. [Google Scholar] [CrossRef] [PubMed]
- Desenclos, J.-C.; Laporte, A.; Brouqui, P. Louse-borne infections in humans. Méd. Mal. Infect. 2011, 41, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Brouqui, P.; Lascola, B.; Roux, V.; Raoult, D. Chronic Bartonella Quintana Bacteremia in Homeless Patients. N. Engl. J. Med. 1999, 340, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Vander Stichele, R.H.; Dezeure, E.M.; Bogaert, M.G. Systematic Review of Clinical Efficacy of Topical Treatments for Head Lice. BMJ 1995, 311, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Chosidow, O.; Chastang, C.; Brue, C.; Bouvet, E.; Izri, M.; Monteny, N.; Bastuji-Garin, S.; Rousset, J. J.; Revuz, J. Controlled Study of Malathion and D-Phenothrin Lotions for Pediculus Humanus Var Capitis-Infested Schoolchildren. Lancet 1994, 344, 1724–1727. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.J. Head Lice. N. Engl. J. Med. 2002, 346, 1645–1650. [Google Scholar] [CrossRef] [PubMed]
- Dodd, C.S. Interventions for Treating Headlice. Cochrane Database Syst. Rev. 2001, 3, CD001165. [Google Scholar] [CrossRef] [PubMed]
- Durand, R.; Bouvresse, S.; Berdjane, Z.; Izri, A.; Chosidow, O.; Clark, J.M. Insecticide Resistance in Head Lice: Clinical, Parasitological and Genetic Aspects. Clin. Microbiol. Infect. 2012, 18, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Bouvresse, S.; Berdjane, Z.; Durand, R.; Bouscaillou, J.; Izri, A.; Chosidow, O. Permethrin and Malathion Resistance in Head Lice: Results of Ex Vivo and Molecular Assays. J. Am. Acad. Dermatol. 2012, 67, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Burgess, I.F.; Brown, C.M.; Lee, P.N. Treatment of Head Louse Infestation with 4% Dimeticone Lotion: Randomised Controlled Equivalence Trial. BMJ 2005, 330, 1423. [Google Scholar] [CrossRef] [PubMed]
- Heukelbach, J.; Pilger, D.; Oliveira, F.A.; Khakban, A.; Ariza, L.; Feldmeier, H. A Highly Efficacious Pediculicide Based on Dimeticone: Randomized Observer Blinded Comparative Trial. BMC Infect. Dis. 2008, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.J.; Casey, D.; Morgan, D.A.; Petrovic, M. Comparison of Wet Combing with Malathion for Treatment of Head Lice in the UK: A Pragmatic Randomised Controlled Trial. Lancet 2000, 356, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Elston, D.M. Controversies Concerning the Treatment of Lice and Scabies. J. Am. Acad. Dermatol. 2002, 46, 794–796. [Google Scholar] [CrossRef] [PubMed]
- Chosidow, O. Bug Buster for Head Lice: Is It Effective? Arch. Dermatol. 2006, 142, 1635–1637. [Google Scholar] [CrossRef] [PubMed]
- Chosidow, A.; Gendrel, D. Safety of oral ivermectin in children. Arch. Pediatr. 2016, 23, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Foucault, C.; Ranque, S.; Badiaga, S.; Rovery, C.; Raoult, D.; Brouqui, P. Oral Ivermectin in the Treatment of Body Lice. J. Infect. Dis. 2006, 193, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Leulmi, H.; Diatta, G.; Sokhna, C.; Rolain, J.-M.; Raoult, D. Assessment of Oral Ivermectin versus Shampoo in the Treatment of Pediculosis (Head Lice Infestation) in Rural Areas of Sine-Saloum, Senegal. Int. J. Antimicrob. Agents 2016, 48, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Lee, S.H.; Kim, J.H. Complete Genome Sequence of the Endosymbiotic Bacterium “Candidatus Riesia Pediculicola”. Microbiol. Resour. Announc. 2021, 10, e01181-20. [Google Scholar] [CrossRef] [PubMed]
- Houhamdi, L.; Parola, P.; Raoult, D. Lice and lice-borne diseases in humans. Med. Trop. 2005, 65, 13–23. [Google Scholar]
- Diatta, G.; Abat, C.; Sokhna, C.; Tissot-Dupont, H.; Rolain, J.-M.; Raoult, D. Head Lice Probably Resistant to Ivermectin Recovered from Two Rural Girls in Dielmo, a Village in Sine-Saloum, Senegal. Int. J. Antimicrob. Agents 2016, 47, 501–502. [Google Scholar] [CrossRef] [PubMed]
- Chosidow, O.; Giraudeau, B. Topical Ivermectin—A Step toward Making Head Lice Dead Lice? N. Engl. J. Med. 2012, 367, 1750–1752. [Google Scholar] [CrossRef] [PubMed]
- Chosidow, O.; Giraudeau, B. Topical Ivermectin Lotion for Head Lice. N. Engl. J. Med. 2013, 368, 968. [Google Scholar] [CrossRef] [PubMed]
- Amanzougaghene, N.; Fenollar, F.; Diatta, G.; Sokhna, C.; Raoult, D.; Mediannikov, O. Mutations in GluCl Associated with Field Ivermectin-Resistant Head Lice from Senegal. Int. J. Antimicrob. Agents 2018, 52, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Sangaré, A.K.; Rolain, J.M.; Gaudart, J.; Weber, P.; Raoult, D. Synergistic Activity of Antibiotics Combined with Ivermectin to Kill Body Lice. Int. J. Antimicrob. Agents 2016, 47, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Diatta, G.; Mediannikov, O.; Sokhna, C.; Bassene, H.; Socolovschi, C.; Ratmanov, P.; Fenollar, F.; Raoult, D. Prevalence of Bartonella Quintana in Patients with Fever and Head Lice from Rural Areas of Sine-Saloum, Senegal. Am. J. Trop. Med. Hyg. 2014, 91, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Boutellis, A.; Veracx, A.; Angelakis, E.; Diatta, G.; Mediannikov, O.; Trape, J.-F.; Raoult, D. Bartonella Quintana in Head Lice from Sénégal. Vector Borne Zoonotic Dis. 2012, 12, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, E.; Rolain, J.-M.; Raoult, D.; Brouqui, P. Bartonella Quintana in Head Louse Nits. FEMS Immunol. Med. Microbiol. 2011, 62, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Coscione, S.; Esau, T.; Kekeubata, E.; Diau, J.; Asugeni, R.; MacLaren, D.; Steer, A.C.; Kositz, C.; Marks, M. Impact of Ivermectin Administered for Scabies Treatment on the Prevalence of Head Lice in Atoifi, Solomon Islands. PLoS Negl. Trop. Dis. 2018, 12, e0006825. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi Open Source Epidemiologic Statistics for Public Health, Version. References Scientific Research Publishing. 2013. Available online: https://www.scirp.org/reference/referencespapers?referenceid=2869128 (accessed on 27 September 2025).
- Raoult, D.; Rolain, J.-M.; Sangare, A.K. Association D’ivermectine et de Composé(s) Antibiotique(s) Pour Un Traitement Thérapeutique Contre Les Poux. WO2016009119A1, 21 January 2016. Available online: https://patents.google.com/patent/WO2016009119A1/fr (accessed on 27 September 2025). [Google Scholar]
- Lynagh, T.; Webb, T.I.; Dixon, C.L.; Cromer, B.A.; Lynch, J.W. Molecular Determinants of Ivermectin Sensitivity at the Glycine Receptor Chloride Channel. J. Biol. Chem. 2011, 286, 43913–43924. [Google Scholar] [CrossRef] [PubMed]
© 2026 Copyright by Authors. Licensed as an open access article using a CC BY 4.0 license.