Afr. J. Parasitol. Mycol. Entomol. , 3(1), 6; doi:10.35995/ajpme03010006
Article
Aspergillus IgG/IgM Seroprevalence Using Aspergillus ICT Test Strips and Immunoblot Assay and Associated Clinical, Radiological, Biological and Microbiological Characteristics
Abdoulaye Kassoum Koné MD PhD 1 ,
Raphaël Piarroux PharmD PhD 2,
Safiatou Niaré Doumbo MD PhD 1,
Abou Coulibaly PharmD 3,
Moctar Coulibaly MD 1,
Aimé Dakoua MD 4,
Souleymane Koné MD 4,
Seydou Karembé MD 4,
Ahmed Konaté MD 1,
Yacouba Toloba MD 4,
Matthew B. Laurens MD PhD 5,
Mahamadou S. Sissoko MD PhD 1,
Abdoulaye Djimdé PharmD PhD 1,
Abdoulaye Dabo PhD 6,
Ogobara K. Doumbo MD PhD 1,†,
Mahamadou Ali Thera MD PhD 1,*
and
Stephane Ranque MD PhD 7,8
,
Raphaël Piarroux PharmD PhD 2,
Safiatou Niaré Doumbo MD PhD 1,
Abou Coulibaly PharmD 3,
Moctar Coulibaly MD 1,
Aimé Dakoua MD 4,
Souleymane Koné MD 4,
Seydou Karembé MD 4,
Ahmed Konaté MD 1,
Yacouba Toloba MD 4,
Matthew B. Laurens MD PhD 5,
Mahamadou S. Sissoko MD PhD 1,
Abdoulaye Djimdé PharmD PhD 1,
Abdoulaye Dabo PhD 6,
Ogobara K. Doumbo MD PhD 1,†,
Mahamadou Ali Thera MD PhD 1,*
and
Stephane Ranque MD PhD 7,8
,
Raphaël Piarroux PharmD PhD 2,
Safiatou Niaré Doumbo MD PhD 1,
Abou Coulibaly PharmD 3,
Moctar Coulibaly MD 1,
Aimé Dakoua MD 4,
Souleymane Koné MD 4,
Seydou Karembé MD 4,
Ahmed Konaté MD 1,
Yacouba Toloba MD 4,
Matthew B. Laurens MD PhD 5,
Mahamadou S. Sissoko MD PhD 1,
Abdoulaye Djimdé PharmD PhD 1,
Abdoulaye Dabo PhD 6,
Ogobara K. Doumbo MD PhD 1,†,
Mahamadou Ali Thera MD PhD 1,*
and
Stephane Ranque MD PhD 7,8
1
Parasites and Microbes Research and Training Center, Faculty of Medicine and Odonto-Stomatology, University of Sciences, Techniques and Technologies of Bamako, International Research Laboratory 3189, Bamako BP:1805, Mali; fankone@icermali.org (A.K.K.); sdoumbo@icermali.org (S.N.D.); coulibalymoctar0879@gmail.com (M.C.); ahmedkonate@icermali.org (A.K.); mssissoko@icermali.org (M.S.S.); adjimde@icermali.org (A.D.); okd@icermali.org (O.K.D.)
2
Efor, Champagne aux monts d’or, France; raphael.piarroux@efor-group.fr
3
Centre d’Infectiologie Charles Mérieux, Bamako, Mali; abouphcie@gmail.com
4
Service de Pneumo-Phtisiologie, Centre Hospitalo-Universitaire du Point G, Bamako, Mali; aime.dakouo17@yahoo.fr (A.D.); diarrhat@yahoo.fr (S.K.); karembeseydou6@gmail.com (S.K.); toloba71@yahoo.fr (Y.T.)
5
Malaria Group, Howard Hughes Medical Institute, Center for Vaccine Development, University of Maryland School of Medicine, Baltimore, MD, USA; mlaurens@som.umaryland.edu
6
Centre National de Recherche Scientifique et Technologique, Bamako, Mali; adabo@icermali.org
7
IHU Méditerranée Infection, 13005 Marseille, France; stephane.ranque@ap-hm.fr
8
IHU Méditerranée Infection, Aix-Marseille Université, AP-HM, IRD, SSA, VITROME, 13005 Marseille, France
*
Corresponding author: mthera@icermali.org; Tel.: +223-76-10-52-89 or +223-66-74-09-61
†
Deceased.
How to cite: Koné, A.K.; Piarroux, R.; Doumbo, S.N.; Coulibaly, A.; Coulibaly, M.; Dakoua, A.; Koné, S.; Karembé, S.; Konaté, A.; Toloba, Y.; et al. Aspergillus IgG/IgM Seroprevalence Using Aspergillus ICT Test Strips and Immunoblot Assay and Associated Clinical, Radiological, Biological and Microbiological Characteristics. Afr. J. Parasitol. Mycol. Entomol. 2025, 3(1): 6; doi:10.35995/ajpme03010006.
Received: 14 March 2025 / Accepted: 17 September 2025 / Published: 18 November 2025
Abstract
: Background: Chronic pulmonary aspergillosis (CPA) occurs in patients with post tuberculosis (TB) sequels. This at-risk population is frequently found in low-resource countries where CPA diagnostic capacity is limited. Characterization of clinical phenotypes using serological tests may help to diagnose the disease. We aimed to assess Aspergillus IgG and its associated factors. Methods: We enrolled 50 adults inpatients and outpatients who were at risk and not at risk of Aspergillosis, from December 2018 to February 2020. Blood and sputum were collected. Aspergillus IgG/IgM antibody was assessed using LDBio Aspergillus ICT Lateral Flow Assay and Aspergillus IgG WB immunoblot assay (LDBio Diagnostics, Lyon, France). Sputum was inoculated on Sabouraud agar medium plus antibiotics (bioMérieux, Marcy-l’Étoile, France), and Aspergillus species were identified using mass spectrometry (Bruker, Billerica, Massachusetts, United States). The association between sociodemographic characteristics, clinical phenotypes, biological parameters and Aspergillosis IgG carriage was assessed. Results: IgG or IgM was detected in 21% of all study participants, 15% and 6%, respectively, in at-risk and not-at-risk participants. Overall, Aspergillus fumigatus was grown in the sputum of 11% of the participants. Chest X-ray showed cavitation in 43%; three cases presented fungal ball evocating an aspergilloma, fibrotic destruction in 17%, nodules in 39%, and variable lesions in 64%. TB chest X-ray abnormalities [OR = 3.3; 95% IC 1.33–10.28] (p = 0.007) or post TB hemoptysis [OR = 4.06, 95% IC 1.34–12.24] (p = 0.01) were risk factors of Aspergillus infection. Conclusions: Cavitation is a common sequel. Aspergillus IgG seroprevalence is high in post TB patients. Aspergillus IgG/IgM determination using a rapid test could help CPA diagnosis at patient point-of-care.
Keywords:
tuberculosis sequels; Aspergillus IgG/IgM; ICT; immunosorbent WB1. Introduction
Aspergillosis is a fungal disease caused by the fungi of the Aspergillus genus; the burden is underestimated in low-income countries mostly due to the limited laboratory diagnosis capacities. Pulmonary Aspergillosis is one of the common complications of post-tuberculosis lung disease [1]. An estimated 372,000 of patients with post TB sequel subsequently developed chronic pulmonary aspergillosis (CPA). CPA prevalence ranges from less than 1 case per 100,000 population in developed Western European countries and the United States of America to 42.9 cases per 100,000 population in Nigeria and the Democratic Republic of Congo [2]. In Mali, few data have been reported on CPA; a single case of CPA in a patient with a history of tuberculosis has been reported in the medical literature [3]. A one-month (8 December 2016, to 8 January 2017) survey of 380 in- and out-patients at the Pneumo-Phthisiology department of the Point G University Hospital in Bamako identified 7 suspected CPA cases, i.e., a 1.8% frequency [Toloba Y, 2017, unpublished data]. A recent estimation of the burden of fungal diseases has shown an estimated prevalence of 7290 cases of chronic pulmonary aspergillosis (often mistaken for TB), with invasive aspergillosis counting for 1230 cases has been reported [4]. CPA diagnosis is based on a combination of clinical, biological, and radiological findings. Mycological diagnosis is complex and laborious with a risk of releasing false-positive fungi cultured from the environment. Detection of Aspergillus IgG is helpful in the laboratory diagnosis of CPA in patients with post tuberculosis disorders [5]. The measurement of titers of Aspergillus antibodies associated with a fungal ball (aspergilloma) on chest X-ray imaging is sufficient to establish a definitive diagnosis of CPA (simple aspergilloma or chronic cavitary aspergillosis depending on the presence of cavitation) [6]. Aspergillosis disease prevalence in sub-Saharan Africa as well as Aspergillus IgG seroprevalence among at-risk patients are underestimated, likely because very few laboratories are equipped to diagnose the disease, and patient point-of-care diagnosis tools are not implemented. The use of a reliable, rapid, inexpensive and sensitive test [7], such as an LDBio Aspergillus ICT Lateral Flow Assay for IgG and IgM detection would help to diagnose and treat suspected cases of CPA in low-income countries. Pulmonary tuberculosis significantly increases the risk of aspergilloma and other CPA [5]. We conducted a study of at-risk and not-at-risk patients of aspergillosis and compared carriers and non-carriers of Aspergillus IgG/IgM (by ICT and WB) to determine the relationship between the socio-demographic characteristics, clinical phenotypes (chest X-ray sequels) and biological parameters with Aspergillus infection in patients attending the Pneumology-Phthisiology department at the Point G Teaching Hospital in Bamako, Mali.
2. Methods
2.1. Study Design, Period and Site
We conducted a cross-sectional study with inpatients, and outpatients at risk and not at risk of Aspergillus infection. Participants were enrolled from December 2018 to February 2020 at the Pneumology-Phthisiology department of Point G Teaching Hospital in Bamako, Mali.
2.2. Inclusion Criteria
At risk participants: Inpatients or outpatients aged from 18 to 70 years old who had post TB chest X-ray abnormalities (sequels) and/or hemoptysis and/or severe chronic obstructive pulmonary disease (COPB) with history of smoking, and/or asthma with Aspergillus sensitization documented by positive skin test and consented to participate in the study were enrolled.
Not-at-risk participants: Inpatients or outpatients aged from 18 to 70 years old seeking care for other diseases without fulfilling any of previously defined criteria for at-risk participants.
2.3. Non-inclusion Criteria
Patients with HIV and CD4+ T-cells with less than 200 cells/µL were not enrolled.
2.4. Sample Collection and Storage
For each participant, the sputum was collected in plastic jars and stored at +4 degree Celsius at Parasites and Microbes Research and Training Center (PMRTC) facilities. Blood was collected in tubes (BD Vacutainer® SST™ Tubes), centrifugated to separate sera, stored at +4 degree Celsius at PMRTC facilities. Sputum was transported at temperature between +4 and +8 °C to Marseille IHU parasitology and mycology laboratory for culture on Sabouraud medium and mass spectrometry analysis. Sera were sent to Lyon, France for Aspergillus IgG and IgM detection using LDBio Aspergillus ICT Lateral Flow Assay for IgG and IgM and the Aspergillus IgG WB immunoblot assay (LDBio Diagnostics, Lyon, France) at temperature between +4 and +8 °C. Sera and sputum were collected from 2018 through 2020, initially stored at PMRTC and then shipped to France in 2021 and 2022. Sample transportation to France was done under strict cold chain maintenance, conform with the study protocol, PMRTC applicable standard operating procedures (SOPs), and international standards using boxes with icepacks and continuous temperature monitoring.
2.5. Culture
Next, 0.5 mL of induced sputum was inoculated onto Sabouraud’s Gentamycin-Chloramphenicol (SGC2 bioMérieux, France) plates and incubated at 30 °C for 5 to 10 days at the Parasitology-Mycology laboratory at University Hospital Institute (IHU) in Marseille, France. Fungal colonies were analyzed macroscopically and fungi were identified using MALDI-TOF mass spectrometry, as previously described by Ranque et al. [8].
2.6. Aspergillus IgG/IgM Detection
Aspergillus IgG/IgM were detected in sera using the Aspergillus ICT IgG-IgM and Aspergillus WB IgG tests (LDBio Diagnostics, Lyon, France). The ICT was performed, as described by Piarroux et al., [9] by depositing 15 µL of serum in the sample well of the cassette and then adding 4 drops of the eluent provided with the kit. The test was then read 20 to 30 min later. If a black band was visible at the test band and a blue band was visible at the control band, the test was positive. If only the control band was visible, the test was negative. If there was no control band, the test was invalid. The WB was performed as described by Oliva et al. [10]. Briefly, 10 µL of serum diluted in 1.2 mL buffer was exposed to a sensitized strip provided in the kit for 90 min, followed by 60 min of incubation in alkaline phosphatase-coupled anti-human IgG buffer, and this was followed by a final incubation in tetrazolium nitroblue-5-Bromo-4-chloro-3-indolyl phosphate solution for 60 min. Interpretation was carried out by comparing incubated samples with the kit’s positive control for bands B16, B18-20, B22 and B30. The presence of at least two of these bands corresponds to a positive test.
2.7. Sample Size Calculation
The sample size was set through a logical decision based on the number of cases of CPA that occurred in a one-month period at the Pneumology department in the Point G Teaching Hospital. We used a prevalence of 1.8% of CPA with an accuracy of 5% and a risk error alpha equal to 5% and a loss of 10% to estimate a sample size of 30 cases of CPA. We then enrolled 50 participants at risk of Aspergillus infection with a history of post TB disorders (chest Rx images of sequelae) or hemoptysis or COPD and 50 not-at-risk participants without those criteria.
2.8. Ethic Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the ethics committee of the University of Science, Techniques and Technologies of Bamako (Approval letter N°2017/109/CE/FMPOS, dated on 17 August 2017. Informed consent was given by each individual participant included in the study.
2.9. Statistical Analysis
The Aspergillus IgG seroprevalence, chest X-ray sequel frequency, and suspected rate of CPA cases were tabulated. The association between sociodemographic characteristics, clinical phenotypes, biological parameters, X-ray chest sequels and Aspergillus IgG was determined using an odds ratio and chi-square test to compare the categorical variable with statistical significance set at p < 0.05.
3. Results
We enrolled at-risk 50 participants and not-at-risk 50 participants; the predominance of males was observed to be 71 (71%), with a sex ratio of 2.5:1 (M:F) and a mean age of 44.6 (±14) years. Aspergillosis IgG seroprevalence by ICT was 21.4% (21/98) [95% CI, 13.8–30.9], and by WB, it was 21.4% (21/98) for WB [95% CI, 13.8–30.9]. Regarding the agreement between ICT and WB, 21 out of 98 participants were ICT-positive and 21 out of 98 participants were WB-positive (Figure 1).
Figure 1.
Study participants’ LDBio Aspergillus ICT Lateral Flow Assay showing positive and negative IgG/IgM.
Figure 1.
Study participants’ LDBio Aspergillus ICT Lateral Flow Assay showing positive and negative IgG/IgM.

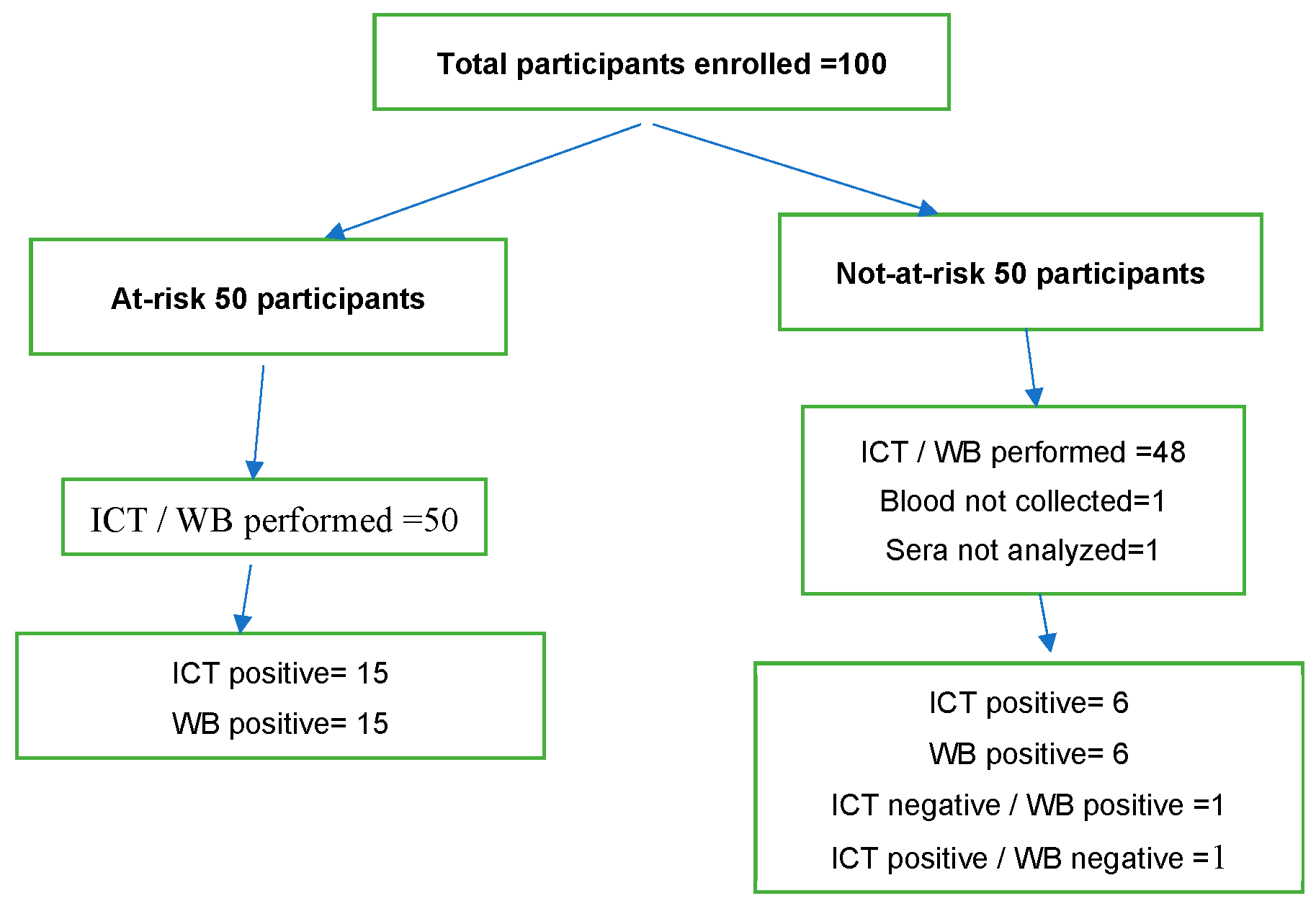
Twenty participants were concomitantly positive for ICT and WB; therefore, one not-at-risk participant was tested negative for WB and positive for ICT and one not-at-risk participant was positive for WB but negative for ICT. ICT and WB tests could not be performed in two participants among the not-at-risk participants because blood was not collected for one and not tested for one (Figure 2).
Figure 2.
Study participants disposition with ICT and WB test performed.
The most common features among the at-risk group were male sex, post TB X-ray chest sequels, hemoptysis in former TB patients, Aspergillus spp. growth from sputum, and ICT/WB-positive patients (Table 1).

Table 1.
Baseline characteristics.
| Participant’s Characteristics | n = 100 | Participants Status at Enrollment | p-Value | |
|---|---|---|---|---|
| At Risk | Not At Risk | |||
| Sex | 0.001 | |||
| Female | 29 (29%) | 7 (7%) | 22 (22%) | |
| Age (years) | 0.44 | |||
| < 40 | 44 (44%) | 28 (28%) | 16 (16%) | |
| TB with Rx pulmonary sequels | 0.0001 | |||
| Yes | 41 (41%) | 40 (40%) | 1 (1%) | |
| Hemoptysis in former TB patients | 0.0001 | |||
| Yes | 18 (18%) | 18 (18%) | 0 (0%) | |
| COPD status | 0.12 | |||
| Yes | 12 (12%) | 9 (9%) | 3 (3%) | |
| Asthma | - | |||
| Yes | 0 (0%) | 0 (0%) | 0 (0%) | |
| HIV status | 0.05 | |||
| Positive | 7 (7%) | 6 (6%) | 1 (1%) | |
| C reactive protein | 0.4 | |||
| Anormal (> 3 mg/dL) | 41 (41%) | 18 (18%) | 23 (23%) | |
| ICT/WB | 0.03 | |||
| Positive | 21 (21%) | 15 (15%) | 6 (6%) | |
| Not performed | 2 (2%) | 0 (0%) | 2 (2%) | |
| Aspergillus spp. | 0.02 | |||
| Yes | 33 (33%) | 17 (17%) | 16 (16%) | |
| Not performed | 13 (13%) | 2 (2%) | 11 (11%) | |
Aspergillus species identification using MALDI-TOF spectrometry: A. fumigatus was detected in the sputum of 11% of the participants among the at-risk group; 66.6% (2/3) of suspected aspergilloma cases were carrying A. fumigatus. A. flavus was found in 4% of study participants. A. niger, A. nidulans, A. oryzae, A. ochraceus and, A. spinulosporus were found in 1% of participants. A. sydowii was detected in 18% of participants, mainly in the not-at-risk group. Other non-Aspergillus fungal species were grown in 24% of participants’ cultures; mass spectrometry was negative in 22% of cases (Table 2).
Table 2.
ICT/WB (IgG-IgM) and mass spectrometry findings (Aspergillus species).
| Aspergillus Species | ICT/WB | ||
|---|---|---|---|
| Negative | Positive | Total | |
| Aspergillus fumigatus | 7 (63.6%) | 4 (36.4%) | 11 (100.0%) |
| Aspergillus flavus | 3 (75.0%) | 1 (25.0%) | 4 (100.0%) |
| Aspergillus nidulans | 1 (100.0%) | 0 (0.0%) | 1 (100.0%) |
| Aspergillus delacroxii | 1 (100.0%) | 0 (0.0%) | 1 (100.0%) |
| Aspergillus niger | 1 (100.0%) | 0 (0.0%) | 1 (100.0%) |
| Aspergillus ochraceus | 1 (100.0%) | 0 (0.0%) | 1 (100.0%) |
| Aspergillus oryzae_CC1 | 1 (100.0%) | 0 (0.0%) | 1 (100.0%) |
| Aspergillus sydowii | 15 (83.3%) | 3 (16.7%) | 18 (100.0%) |
| Other fungal species | 8 (80.0%) | 2 (20.0%) | 10 (100.0%) |
| Negative culture | 21 (84.0%) | 4 (16.0%) | 25 (100.0%) |
| No samples (sputum) | 18 (72.0%) | 7 (28.0%) | 25 (100.0%) |
| Total | 77 (78.6%) | 21 (21.4%) | 98 (100.0%) |
Suspected aspergilloma (cavitation + fungal ball with or without positive ICT/WB IgG) was seen in three participants (3%); cured TB patients who had ICT/WB positive represented 12% (Table 3).
Table 3.
Clinical phenotype frequencies.
| Clinical Phenotypes | Number | Frequency |
|---|---|---|
| Suspected aspergilloma | 3 | 3% |
| Cured TB with positive WB/ICT | 12 | 12% |
| Empirical Bacterial infection or active TB (WB/ICT positive +) | 6 | 6% |
| Others with negative WB/ICT | 79 | 79% |
| Total | 100 | 100% |
ICT: Immunochromatographic Technology, WB: Western blot, TB: Tuberculosis.
Chest X-ray with sequels, hemoptysis and Aspergillus spp. growth from sputum were frequent in Aspergillus IgG antibody carriers. Positive HIV status, asthma, abnormal C-reactive protein and Chronic obstructive pulmonary disease (COPD) were not associated with Aspergillus IgG (Table 4).
Table 4.
Association between sociodemographic, clinical and biological parameters and ICT/WB.
| Participants Characteristics at Enrollment | n = 98 | ICT/WB | p-Value | |||
|---|---|---|---|---|---|---|
| Positive | Negative | OR | 95% IC | |||
| Sex | 0.69 | 0.22–2.1 | 0.17 | |||
| Female | 29 (29.6%) | 5 (5.1) | 24 (24.5) | |||
| Age (years) | 1.05 | 0.39–2.79 | 0.19 | |||
| <40 | 43 (43.9%) | 9 (9.1%) | 34 (34.7%) | |||
| TB chest X-ray sequels | 3.3 | 1.33–10.28 | 0.007 | |||
| Yes | 41 (41,9%) | 14 (14.2%) | 27 (27.5%) | |||
| Hemoptysis former TB | 4.06 | 1.34–12.24 | 0.01 | |||
| Yes | 18 (18.3%) | 8 (8.16%) | 10 (10.2%) | |||
| COPD status | 0.79 | 0.15–3.9 | 0.56 | |||
| Yes | 11 (11.2%) | 2 (2.04%) | 9 (9.18%) | |||
| Asthma | - | – | - | |||
| Yes | 0 (0%) | 0 (0.0%) | 0 (0.0%) | |||
| HIV status | 1.51 | 0.27–8.43 | 0.4 | |||
| Positive | 6 (6.12%) | 2 (2.04%) | 4 (4.08) | |||
| C reactive protein | 0.79 | 0.28–2.21 | 0.18 | |||
| Anormal (>3 mg/dL) | 41 (41.9%) | 8 (8.16%) | 33 (33.6%) | |||
| Aspergillus spp. | - | - | 0.06 | |||
| Yes | 33 (33.6%) | 5 (5.1%) | 28 (28.5%) | |||
| Not performed | 13 (13.2%) | 11 (11.2%) | 2 (2.04%) | |||
CRP: C Reactive Protein; ICT: Immunochromatographic Technology, COPD: chronic obstructive pulmonary disease, TB: Tuberculosis.
Chest X-ray sequel characteristics among participants were pulmonary cavitation with a fungal ball identified in three participants, confirming a suspected aspergilloma. Aspergillus IgG was detected in two suspected aspergilloma. Fibrotic destruction was seen in 16.3%, nodules in 38.7%, variable pulmonary sequels in 63.2%, and radiological progression in 4.08% (Table 5). Participants with suspected CPA are also those who had fibrotic destruction and radiological variable sequels (Table 5).
Table 5.
Association between pulmonary sequels characteristics, clinical and biological parameters, and LDBio ICT/WB Aspergillus IgG/IgM-positive tests.
Table 5.
Association between pulmonary sequels characteristics, clinical and biological parameters, and LDBio ICT/WB Aspergillus IgG/IgM-positive tests.
| TB Chest Radiological Sequelae Characteristics | n = 98 | ICT/WB | p-Value | |||
|---|---|---|---|---|---|---|
| Negative | Positive | OR | 95% IC | |||
| Cavities with fungal ball | 0.18 | 0,12–0.28 | 0.009 | |||
| Yes | 3 (3.06%) | 0 (0.0) | 3 (3.06%) | |||
| Fibrotic destruction | 3.77 | 1.20–11.84 | 0.02 | |||
| Yes | 16 (16.3% | 9 (9.18%) | 7 (7.14%) | |||
| Nodules | 0.96 | 0.37–2.7 | 0.19 | |||
| Yes | 38 (38.7%) | 30 (30.6%) | 8 (8.1) | |||
| Variables radiological sequels | 0.43 | 0.16–1.16 | 0.05 | |||
| Yes | 62 (63.2%) | 52 (35.6%) | 10 (10.2%) | |||
| Radiological progression | 1.2 | 0.12–12.50 | 0.6 | |||
| Yes | 4 (4.08%) | 3 (3.06) | 1 (1.02) | |||
4. Discussion
This study is pioneering in its investigation of aspergillosis seroprevalence in patients who are at risk of and not at risk of aspergillosis in a hospital setting in Mali. The seroprevalence of Aspergillus IgG and prevalence of CPA were studied in different population subgroups and settings using qualitative and quantitative tests [11,12,13]. The prevalence of suspected cases of CPA (aspergilloma) and the seroprevalence of Aspergillus IgG among study participants would indicate that Aspergillus infection is common in Malian adult patients, as suggested by Niaré-Doumbo et al. [4]. As previously published [9,14], we found a substantial agreement between ICT and WB results. The overall prevalence of suspected (possible) aspergilloma in our post TB patients with chest X-ray sequels (pulmonary cavities) matched previously reported cases; CPA was reported to develop commonly in post TB pulmonary cavitation [15], which is the common post pulmonary TB sequel [16]. Therefore, other post TB pulmonary sequels, such as fibrotic destruction and variable radiological sequels were found to be associated with Aspergillus IgG/IgM in our study; these chest radiography characteristics are recognized among the imaging spectrum of CPA [17]. In Seoul, South Korea [18], 2.9% of the 345 patients diagnosed, treated, and followed-up until TB was cured developed chronic pulmonary aspergillosis. The prevalence of aspergilloma was higher in patients with a history of treatment of pulmonary TB [19]. CPA may develop in newly diagnosed pulmonary TB patients at diagnosis and during anti-tubercular treatment, with increasing CPA prevalence during the treatment course [20]. In our study, Aspergillus IgG seroprevalence was two-fold higher in at-risk participants than in not-at-risk participants. This result highlights that exposition to Aspergillus spp. infection is high and the risk of infection increases in patients with post TB disorders in low-income countries. Similar variations in Aspergillosis IgG seroprevalence among healthy volunteers, TB close contacts, active TB patients and old TB cases with 33.0% (66/200), 37.7% (123/326), 26.5% (139/524) and 43.2% (83/192), respectively, were found by Lee et al. in 2020 in Taiwan using ImmunoCAPTM system [12]. Considering the seroprevalence of Aspergillus IgG among our study patients with post TB chest X-ray sequels, we assume both tests evaluated in our study could be useful for suspected CPA screening in high-TB-endemic, low-income countries such as Mali. The difference observed between both studies could be linked to the sensitivity of the ImmunoCAPTM system, post TB prevalence, and the criteria used to enroll at-risk participants in our study.
Men were more frequently enrolled than women in both groups; this could explain why men were carrying more Aspergillus IgG than women; male predominance has been reported by several authors [7,11].
A study conducted in Mozambique in individuals treated for and cured from tuberculosis showed that 3 out of 61 (5%) had Aspergillus-specific IgG detected using automated Immunocapture® (Phadia 100, Thermo Fisher Scientific, Uppsala, Sweden); the HIV-positive patients included in this study had no detectable levels of anti-Aspergillus antibodies [11]. Our findings are consistent with the Mozambican study; in the present study, for both ICT and WB, HIV-positive patients were Aspergillus IgG-negative. The use of ICT/WB may not be helpful to screen aspergillosis in HIV-positive patients with post TB chest radiography abnormalities.
Aspergillus spp. are frequently identified in samples collected in confirmed CPA cases, Hunter et al. found 36% carriers of A. fumigatus among confirmed CPA cases [7]. The growth of Aspergillus spp. in patients’ sputum with chest radiography sequels associated with the Aspergillus IgM (LDBio IgG/IgM positive) in the present study can confirm active Aspergillus infection, as more than half of the suspected aspergilloma cases had A. fumigatus isolated from culture.
Niaré-Doumbo et al. found A. fumigatus in 3% of cases, and A. niger was the predominant species (29%) in the sputum and the nasal swabs from inpatients at the oncology-hematology department in Point G Teaching Hospital [4]; this result is not consistent with what we found because the characteristics of our patients’ illnesses were different from those from Niaré-Doumbo et al.’s study. Hunter et al. reported A. fumigatus as the most prevalent species in CPA patients [7], and this finding is consistent with what we found in the current study. Variation in Aspergillus species circulating in hospital wards and their frequency could be dependent on inpatients’ disorders instead of ward characteristics.
One study limitation is the lack of confirmation of CPA diagnosis using antibody titer measurements; therefore, the at-risk participants with chest X-ray abnormalities associated with Aspergillus IgG/IgM using ICT test strips and immunoblot assays could be considered as possible CPA. An assessment of IgG titers is needed for the confirmation of suspected cases.
5. Conclusions
Our findings suggest that anti-Aspergillus fumigatus IgG/IgM carriage is common in post-TB patients in Mali. The detection of anti-Aspergillus antibodies using ICT is well adapted to laboratories with limited resources in highly exposed patients in endemic TB countries. Our findings advocate for making this diagnostic test available in low-income countries such as Mali to enhance the screening of aspergillosis, a life-threatening disease. Confirmation tests determining antibody titers should be implemented for the purpose of CPA diagnosis and treatment.
Author Contributions
O.K.D., S.R., M.A.T., A.K.K., R.P., Y.T, S.N.D., A.D (Abdoulaye Dabo). contributed to the study conception and design. The data collection was carried out by A.C., M.C., S.K (Souleymane Koné), SK (Seydou Karembé)., Mycological and mass spectrometry analysis were performed by A.K, A.K.K. and S.R. Serological tests were performed by R.P. The preparation of the material and data analysis were carried out by M.S.S., A.K.K., R.P., S.R., A.D., (Aimé Dakoua), M.C., and M.A.T. The first draft of the manuscript was written by A.K.K., the review by R.P., S.R., A.D., (Abdoulaye Dabo)., M.A.T., A.D., (Abdoulaye Djimdé), Y.T., S.N.D., and M.B.L. All authors have read and agreed to the published version of the manuscript.
Funding
The IHU Méditerranée Infection in Marseille supported the mycological and mass spectrometry analysis. The laboratory LDBio Diagnostics, Lyon, France, supported the ICT and WB tests for the serological analyses and the International Research Laboratory 3189/Malaria Research and Training Center provided the funds allocated for the recruitment of study participants.
Acknowledgments
We thank the staff of Point G Teaching Hospital’s Pneumology-Phthisiology department for the effort made in recruiting patients.
Conflicts of Interest
RP was employed by LDBIO Diagnostics at the time of the study. All other authors declare that they have no competing interests.
References
- van Kampen, S.C.; Wanner, A.; Edwards, M.; Harries, A.D.; Kirenga, B.J.; Chakaya, J.; Jones, R. International research and guidelines on post-tuberculosis chronic lung disorders: A systematic scoping review. BMJ Glob. Health 2018, 3, e000745. [Google Scholar] [CrossRef] [PubMed]
- Denning, DW.; Pleuvry, A.; Cole, DC. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Dao, S.; Diallo, S.; Maiga, I.; Sissoko, F.; Kayantao, D. Aspergillose pulmonaire chez un ancien tuberculeux en milieu spécialisé de Bamako. Mali. Med. 2005, 20, 54–55. [Google Scholar] [PubMed]
- Niaré-Doumbo, S.; Normand, A.C.; Diallo, Y.L.; Dembelé, A.K.; Thera, M.A.; Diallo, D.; Piarroux, R.; Doumbo, O.; Ranque, S. Preliminary study of the fungal ecology at the haematology and medical-oncology ward in Bamako, Mali. Mycopathologia 2014, 178, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Denning, DW.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [PubMed]
- Hunter, E.S.; Page, I.D.; Richardson, M.D.; Denning, D.W. Evaluation of the LDBio Aspergillus ICT lateral flow assay for serodiagnosis of allergic bronchopulmonary aspergillosis. PLoS ONE 2020, 15, e0238855. [Google Scholar] [CrossRef] [PubMed]
- Ranque, S.; Normand, A.C.; Cassagne, C.; Murat, J.B.; Bourgeois, N.; Dalle, F.; Gari-Toussaint, M.; Fourquet, P.; Hendrickx, M.; Piarroux, R. MALDI-TOF mass spectrometry identification of filamentous fungi in the clinical laboratory. Mycoses 2014, 57, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Piarroux, R.P.; Romain, T.; Martin, A.; Vainqueur, D.; Vitte, J.; Lachaud, L.; et al. Multicenter Evaluation of a Novel Immunochromatographic Test for Anti-aspergillus IgG Detection. Front. Cell Infect. Microbiol. 2019, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Flori, P.; Hennequin, C.; Dubus, J.C.; Reynaud-Gaubert, M.; Charpin, D.; Vergnon, J.M.; Gay, P.; Colly, A.; Piarroux, R.; et al. Evaluation of the Aspergillus Western blot IgG kit for diagnosis of chronic aspergillosis. J. Clin. Microbiol. 2015, 53, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Salzer, H.J.F.; Massango, I.; Bhatt, N.; Machonisse, E.; Reimann, M.; Heldt, S.; Lange, C.; Hoelscher, M.; Khosa, C.; Rachow, A. Seroprevalence of Aspergillus-Specific IgG Antibody among Mozambican Tuberculosis Patients. J. Fungi 2021, 7, 595. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Huang, HL.; Chen, L.C.; Yang, H.C.; Ko, J.C.; Cheng, M.H.; Chong, I.-W.; Lee, L.-N.; Wang, J.-Y.; Dimopoulos, G. Seroprevalence of Aspergillus IgG and disease prevalence of chronic pulmonary aspergillosis in a country with intermediate burden of tuberculosis: A prospective observational study. Clin. Microbiol. Infect. 2020, 26, e1–e1091. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Chang, H.L.; Chen, Y.H.; Liu, C.J.; Keng, L.T.; Huang, H.L.; Wang, J.-Y.; Sheu, C.-C.; Chong, I.-W. Seroprevalence and prognostic value of Aspergillus-specific IgG among non-neutropenic invasive pulmonary aspergillosis patients: A prospective multicenter study. Pneumonia 2024, 16, 28. [Google Scholar] [CrossRef]
- Rozaliyani, A.; Setianingrum, F.; Azahra, S.; Abdullah, A.; Fatril, A.E.; Rosianawati, H.; Burhan, E.; Handayani, D.; Arifin, A.R.; Zaini, J.; et al. Performance of LDBio Aspergillus WB and ICT Antibody Detection in Chronic Pulmonary Aspergillosis. J. Fungi 2021, 7, 311. [Google Scholar] [CrossRef] [PubMed]
- Page, ID.; Richardson, M.D.; Denning, D.W. Comparison of six Aspergillus-specific IgG assays for the diagnosis of chronic pulmonary aspergillosis (CPA). J. Infect. 2016, 72, 240–249. [Google Scholar] [CrossRef]
- Hedayati, M.T.; Azimi, Y.; Droudinia, A.; Mousavi, B.; Khalilian, A.; Hedayati, N.; Denning, D.W. Prevalence of chronic pulmonary aspergillosis in patients with tuberculosis from Iran. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1759–1765. [Google Scholar] [CrossRef]
- Garg, M.; Bhatia, H.; Chandra, T.; Debi, U.; Sehgal, IS.; Prabhakar, N.; Sandhu, M.S.; Agarwal, R. Imaging Spectrum in Chronic Pulmonary Aspergillosis. Am. J. Trop. Med. Hyg. 2023, 108, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Moon, J.W.; Park, Y.B.; Ko, Y. Serological Changes in Anti-Aspergillus IgG Antibody and Development of Chronic Pulmonary Aspergillosis in Patients Treated for Pulmonary Tuberculosis. J. Fungi 2022, 8, 130. [Google Scholar] [CrossRef] [PubMed]
- Lakhtakia, L.; Spalgais, S.; Kumar, R. Spectrum of pulmonary Aspergillus diseases in post TB lung diseases. Indian. J. Tuberc. 2022, 69, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Jha, D.; Kumar, U.; Meena, V.P.; Sethi, P.; Singh, A.; Nischal, N.; Jorwal, P.; Vyas, S.; Singh, G.; Xess, I.; et al. Chronic pulmonary aspergillosis incidence in newly detected pulmonary tuberculosis cases during follow-up. Mycoses 2024, 67, e13747. [Google Scholar] [CrossRef] [PubMed]
© 2025 Copyright by Authors. Licensed as an open access article using a CC BY 4.0 license.